February 2006, Vol 28, No. 2 |
Update Articles
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
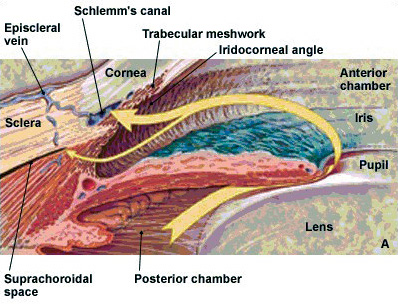
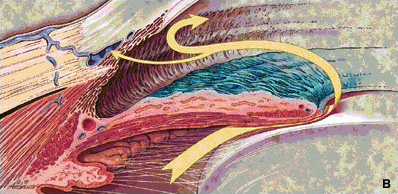
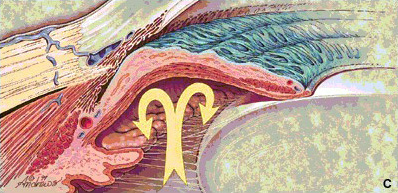
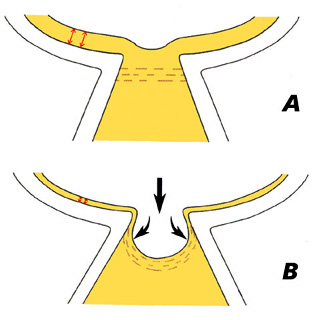
Glaucoma - An update and overview on classification and managementJackson Woo 胡澤燊 HK Pract 2006;28:76-84 Summary Most glaucoma patients have no symptoms and quite often their disease are only suspected or confirmed during routine eye screening. It is a slowly progressive condition in which the retinal nerve fibers degenerate. If untreated, blindness is almost invariable although the time course and speed vary. Up to the current moment, intraocular pressure reduction is the only effective mechanism of treatment by which the disease process can be slowed or stopped. The role of neuro-protection medications is still uncertain. 摘要 大多數的青光眼病人沒有任何症狀,通常是眼科常規檢查時被懷疑或確診患有該病。青光眼是視網膜神經慢性的進行纖維退變。若未經治療,就會導致失明,雖然病程和失明的速度有所不同。到目前為止,降低眼壓(IOP reduction)是唯一可減緩或終止疾病過程的有效機制。神經保護藥物的作用尚不清楚。 Introduction Glaucoma is a heterogeneous group of ocular diseases that manifest as a progressive optic neuropathy and visual loss.1,2 Visual field loss and even irreversible blindness occur if glaucoma is not appropriately diagnosed and treated. Despite the availability of intraocular pressure (IOP) lowering agents that may arrest or slow disease progression, glaucomatous blindness still occurs. Acute angle-closing glaucoma can be considered to be a separate entity in which patients may not have any visual field defects or high IOP before the attack. It happens in individuals who have occludable angles as a result of naturally-occurring or acquired abnormal anatomy of the angle structures. During the acute attack, patients have symptoms of severe ocular pain and headache, blurring of vision and nausea and vomiting as a result of rapidly increasing IOP. Even with effective medical and laser treatment, some of these acute cases may eventually end up in some forms of chronic angle- closure glaucomas, the consequences of which may be similar to those of the chronic open-angle types. The main focus of this paper concentrates on the various clinical aspects of the latter. The nature and burden of glaucoma Most glaucomas are insidious in nature, with no symptoms or warning signs prior to advanced visual field loss.1,2 At least half of the patients with open-angle glaucoma are not receiving treatment because the disease is undiagnosed.1,3-6 Among treated glaucoma patients, poor compliance is a major obstacle.2,7,8 It is estimated that 6.7% of the 67 million people with glaucoma worldwide5 - and 120,000 of the 3 million people afflicted with it in the United States1 - are blind as a result. Glaucoma is a significant public health problem. In the United States alone, glaucomatous blindness costs an estimated US$1.5 billion annually in Social Security benefits, lost income tax revenues, and healthcare expenditures.9 Added to the economic burden imposed by blindness is the impact on patients' lives. Even before blindness occurs, patients diagnosed with and treated for glaucoma may be troubled by treatment inconvenience and the fear of vision loss. Epidemiology of glaucomaGlaucomatous optic neuropathy is most prevalent among people of African origin, and least prevalent in full-blooded Australian aborigines;10 Asian populations have rates intermediate between theses two groups. European- and African- derived peoples suffer predominantly from primary open-angle glaucoma (POAG), whereas rates of primary angle-closure glaucoma (PACG) are higher among East Asians than in other populations. Glaucoma as a cause of blindness Population surveys in Mongolia found glaucoma to be the cause of 35% of blindness in adults (cataract being the cause of 36% of blindness).11 Among Chinese Singaporeans, 60% of adult blindness was caused by glaucoma.12 Cautious extrapolation of these data suggests that around 1.7 million people in China suffer blindness caused by glaucoma. PACG is responsible for the vast majority (91%) of these cases.13 Secondary glaucoma is the most common cause of uniocular blindness. Glaucoma is the leading cause of registered, permanent blindness in Hong Kong (23%).14 In Japan, diabetic retinopathy (18%), cataract (16%) and glaucoma (15%) are the leading causes of blindness.15 Risk factors for glaucoma Apart from high IOP's, advancing age is the single most consistent risk factor for all types of glaucoma.12,16-23 A positive family history is also a risk factor for glaucoma.24,25 Female gender is recognized as a major predisposing factor toward the development of PACG.12,20,23 There is little clear evidence to support a gender difference in POAG. Those of Chinese ethnic origin are at a higher risk of developing angle-closure glaucoma than those of Malay descent and South Indian people.16,17 All the above and in particular raised IOP have been shown by Foster et al in a recent Singaporean Study to be risk factors for glaucomatous optic neuropathy in Chinese people.26 A shallow anterior chamber has long been recognized to be a factor that predisposes toward angle-closure.27 The depth of the anterior chamber reduces with age and tends to be shallower in women than in men.28,29 There may also be an association between myopia and POAG.30 Other risk factors are diabetes mellitus, hypertension and a thin central corneal thickness (<0.5mm). Intraocular pressure and glaucoma progression As mentioned above, glaucoma does not refer to a single disease entity, but rather to a group of diseases that have certain common features, including high IOP (too high for the continued health of the eye), cupping and atrophy of the optic nerve head, and visual field loss. IOP is determined by three factors: (a) the rate of aqueous humor production by the ciliary body, (b) the resistance to aqueous outflow across the trabecular meshwork - Schlemm's canal system, and (c) the level of episcleral venous pressure. In most cases, increased IOP is caused by increased resistance to aqueous humor outflow; in a minority of cases, elevated IOP is caused by increased episcleral venous pressure. Although the causes of glaucoma are still unknown, studies suggest controlling IOP slows the risk of disease progression.31,32 In fact, elevated IOP is considered to be one of the most important risk factors for glaucoma.2,3,6 Classification The many types of glaucoma are classified, primarily, as being of (a) the open-angle or (b) angle-closure type, according to the manner in which aqueous outflow is impaired. In open-angle glaucoma, the elevation in IOP is caused by increased resistance in the drainage channels; whereas in angle-closure glaucoma the obstruction to aqueous outflow is caused by closure of the chamber angle by the peripheral iris.
Further classification describes the disorder as (a) primary or (b) secondary depending on the absence or presence of associated factors contributing to the IOP rise (e.g., presence of proliferative diabetic retinopathy and uveitis, use of topical steroids and following trauma). In some cases, the age of the patient at the onset of glaucoma is also taken into consideration and the condition is then described as congenital, infantile, juvenile, or adult accordingly. Assessment A full assessment will be preformed by an ophthalmologist once he/she suspects the patient is suffering from glaucoma. The aims of the initial assessment are:
Intraocular pressure The IOP is measured by various kinds of tonometers, the gold standard of which is called Goldmann Tonometer. It is usually a kind of slit-lamp mount instrument and designed in a way that the IOP can easily be measured at the same time as the routine slit-lamp biomicroscopic eye examination. Unfortunately there is no safe safety-margin below which any eye can be free of glaucomatous damage. The figure of 21.5 mmHg is a by-product of statistics (mean+/-standard deviations) using old Western data base. However, in general, the higher the IOP is, the more is the likelihood of the presence of glaucomatous damage to an eye. Gonioscopy Gonioscopy is crucial for the proper diagnosis of glaucoma. Furthermore, it is essential for glaucoma treatment in the angle (e.g., laser trabeculoplasty). Gonioscopy should be performed on all patients with glaucoma, on all glaucoma suspects, and on all individuals thought to have narrow angles. Proper management of glaucoma requires that the clinician determine whether the angle is open or closed. In angle-closure, the peripheral iris obstructs the trabecular meshwork, (i.e., the meshwork is not visible on gonioscopy). The width of the angle is determined by the site of insertion of the iris on the ciliary face, the convexity of the iris, and the prominence of the peripheral iris roll. If the angle between the peripheral iris and the trabecular meshwork exceeds 20o, angle-closure is unlikely. Optic nerve head morphology Ophthalmoscopy is used to examine the inside of the eye, especially the optic nerve. Glaucomatous damage typically appears as cupping or increased cup-to- disc area ratio. The cup is classically defined as the white central part of the optic nerve head (optic disc). The usual average optic disc diameter is about 1.5mm. A cup with a diameter of more than 0.5mm (resulting in a cup-to-disc ratio of more than 0.3) is generally considered to be a feature of glaucoma suspects.
In recent years, three new techniques of optic nerve imaging have become widely available. These are (a) scanning laser polarimetry (GDx), (b) confocal laser ophthalmoscopy (Heidelberg Retinal Tomography or HRT), and (c) optical coherence tomography (OCT). The GDx machine does not actually image the optic nerve but rather it measures the thickness of the nerve fiber layer on the retinal surface just before the fibers pass over the optic nerve margin to form the optic nerve. The HRT scans the retinal surface and optic nerve with a laser. It then constructs a topographic (3-D) image of the optic nerve including a contour outline of the optic cup. The nerve fiber layer thickness is also measured. The OCT instrument utilizes a technique called optical coherence tomography which creates images by use of special beams of light. The OCT machine can create a contour map of the optic nerve, optic cup and measure the retinal nerve fiber thickness. Over time all three of these machines can detect loss of optic nerve fibers. Perimetry Perimetry is performed with either static or kinetic presentations of the target. Kinetic perimetry (e.g., Goldmann) uses a moving stimulus of fixed intensity. The stimulus is moved at a steady rate from a non-seeing area to a seeing area until it is perceived by the patient. Static perimetry (Humphrey) uses a stationary stimulus of variable intensity. The intensity is increased until the patient first recognizes the presence of the stimulus.
It is important to correlate changes in the visual field with those in the optic nerve head. If an appropriate correlation is not present, other causes of visual loss must be considered, (e.g., ischaemic optic neuropathy, demyelinating disease, pituitary tumor, etc.) TreatmentThe objective of glaucoma treatment is to maintain functional vision throughout the patient's lifetime with minimal effect on quality of life. The goal of intervention is risk factor reduction:
Angle control There are some situations (PACG and chronic narrow-angle or angle-closure glaucoma) in which treatment at the angle or structures near-by may be beneficial. Pilocarpine has the effect of contracting the longitudinal part of the ciliary muscles and thus helps re-opening a closed angle. In cases of acute angle-closure glaucoma or narrow-angle glaucoma, a laser iridotomy (LI) or a laser iridoplasty also helps re-opening a closed angle and reduces the chance of further angle-closure from happening. Paediatric glaucomas can sometimes be controlled well with a goniotomy. But actually it is a drainage procedure although the primary site of interest is the angle. There are some situations in which a very swollen cataract may push the iris forward and occlude the angle. In those cases, a simple cataract surgery may cure the disease.
Reducing IOP Studies suggest that lowering IOP can help to slow or stop the likelihood of disease progression.31,32 IOP can be lowered by reducing the production of aqueous humor or increasing its drainage "out" of the eye33-35 via (a) medical treatment, (b) laser therapy or (c) surgery.6,7,33,35,36 Despite wide differences in practice patterns,36 monotherapy with a topical beta-adrenergic receptor antagonist (beta-blocker) has attained global acceptance as standard first-line therapy for POAG.6,34,35,37-39 Unfortunately, topical beta-blockers may not be a long-term solution. According to a multinational observational study, approximately 50% of patients with POAG or ocular hypertension required either additional medication or a switch from beta-blocker therapy within 2 years of treatment initiation.40 These patients with hypertension have high IOP but there are no cupping of the disc or visual field defect. A certain portion of them eventually develop other glaucoma features. Some ophthalmologists regard ocular hypertension as an early state of glaucoma. Inability to control IOP was the most frequently cited reason for treatment change. Side effects also hampered the long-term usefulness of nonselective beta-blocker monotherapy.
With the exception of the United Kingdom and the Netherlands, where more patients undergo laser trabeculoplasty or trabeculectomy after failure of first-line therapy, the preferred second-line therapy after beta-blocker monotherapy is either a different monotherapy or combination therapy. Switching to a different monotherapy is generally recommended before resorting to combination therapy.6,39 Laser and surgical procedures are usually used only after medical treatment has failed.2,7,33
Argon laser trabeculoplasty (ALT) is a common treatment procedure for the treatment of POAG in the West. The laser beam opens the fluid channels (trabeculum) of the eye, helping the drainage system to work better. In many cases, medication will still be needed. Usually, half the trabeculum is treated first. If necessary, the other half can be treated in a separate session another time. This method prevents over-correction and lowers the risk of increased pressure following surgery. ALT has successfully lowered IOP in up to 75% of patients treated.
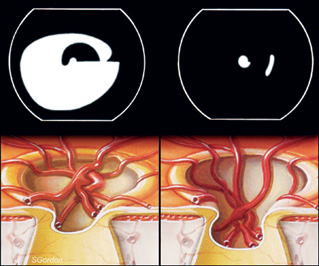
Selective laser trabeculoplasty (SLT) is a new form of trabeculum laser treatment under multi-center clinical trials. It uses a combination of laser frequencies that allow the laser to work at very low levels. It treats specific cells "selectively", leaving untreated portions of the trabeculum intact. For this reason, it is believed that SLT, unlike other types of laser surgery, may be safely repeated many times. Cyclophotocoaguation (YAG or Diode laser) is a "last-ditch" procedure to save an eye from severe glaucoma damage not managed by standard glaucoma surgery. This surgery destroys part of the ciliary body, the part of the eye that produces intraocular fluid. This procedure may need to be repeated in order to permanently control glaucoma. Trabeculectomy may be needed in cases in which both medical and/or laser treatments fail to lower the IOP to the target level. In this filtering microsurgery, a tiny drainage hole is made in the sclera (under a pre-opened partial thickness scleral flap). If successful, the hole will act as a fistula through which the aqueous humor flows from the anterior chamber into the sub-conjunctival space, bypassing the highly resistant trabecular meshwork. As a result, the IOP can be lowered to a level at which retinal nerve fiber damage is minimized.
In general, glaucoma filtering surgery is successful in about 70-90% of cases. Occasionally, the surgically created drainage fistula begins to close (wound healing) and the IOP rises again. This occurs most often in younger patients. Anti-wound healing drugs, such as mitomycin-C and 5-FU, help to slow down the "healing". If needed, trabeculectomy can be done a number of times in the same eye (usually at different sites). Glaucoma drainage devices are intraocular implants which allow aqueous to flow from the anterior chamber into a maintained episcleral space from where it can be absorbed into surrounding blood vessels. There are a few commercial preparations in the market, such as Molteno, Ahmed, Baerveldt, etc. It is indicated when there is a very high risk of failure of trabeculectomy even with anti-fibrotics - these eyes invariably have severe, refractory glaucoma:
This surgery, and the management of the patient post-operatively is complicated. Only an ophthalmologist with appropriate training and experience in glaucoma should perform it. Conclusion Life-long medical and ophthalmological follow up is necessary with or without a good disease control. As a result of its chronic nature, a good drug compliance and trusting doctor-patient relationship is essential in achieving the ultimate objective: "To maintain functional vision throughout the patient's lifetime with minimal effect on quality of life." Key messages
Jackson Woo, FRCS(Glasg),
FHKAM(Ophthal) Correspondence to: Dr Jackson Woo, Department of Ophthalmology, Caritas Medical Centre, 111 Wing Hong Street, Sham Shui Po, Kowloon. References
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||