|
December 2009, Volume 31, No. 4
|
Case Report
|
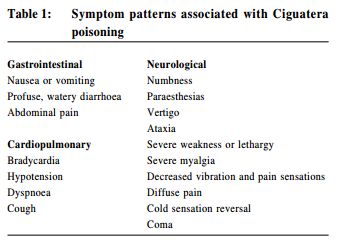
Case report on ciguatera poisoningHon-ho Sze施漢豪, Wendy WS Tsui 徐詠詩 HK Pract 2009;31:199-201 Summary In Hong Kong, ciguatera fish poisoning is not unfamiliar to us. It can cause gastrointestinal, neurological and/or cardiopulmonary symptoms several hours after consumption of toxic fish. The treatment is mainly supportive. Certain medications, e.g. atropine, calcium gluconate, amitriptyline and mannitol, might be used in specific cases. Minor cases could be managed in the community. Family physicians can also play an active role in public education about prevention of ciguatoxin poisoning. 摘要 雪卡毒中毒在香港並不少見。在進食毒魚後數小時,可引 致消化系統,神經系統和/或心肺系統的症狀。治療主要為支 援性質,特殊病例可採用阿托品、葡萄酸鈣、阿米替林和甘露 醇來治療。輕微症狀的個案,可在社區內治療。家庭醫生在教 育公眾關於預防雪卡毒中毒方面,可起積極的作用。 Introduction Acute gastro-intestinal symptoms are common daily presenting complaints in primary care. As a family physician, we need to make an appropriate diagnosis and provide justifiable management. Patients with an acute abdomen should be referred without hesitation. Of course, most cases are self-limiting and can be treated conservatively. We would like to report a case which family physicians could manage at their clinic most of the time. In Hong Kong, coral reef fishes are not unfamiliar to us. Hong Kong people enjoy eating them especially at our local banquets, even though some of the species are facing extinction and consumers may risk ciguatera poisoning. While the ciguatoxin does not cause harm to marine fish, ingestion by humans may result in health consequences. Case Report A 51-year-old lady presented to our clinic with diarrhoea, toothache and left jaw pain after taking a superlarge carol reef fish four days ago. She also had associated tiredness, myalgia, tongue numbness and loose stool. There was no per rectal bleeding. Apart from mild abdominal bloating, she had no nausea, vomiting, nor abdominal pain. Family members who had attended the dinner were all affected, including her father, brothers, and some other relatives. They had already reported the incident to the Department of Health. For this consultation, she expected pain relief as the jaw pain was not controlled by paracetamol alone. On physical examination, her general condition and hydration status was good. There was neither tongue nor buccal lesions. The abdomen was soft and non-tender. The impression was ciguatera poisoning. The patient was prescribed with dologesic for symptomatic relief. The patient was followed up the next day. The diarrhoea, tiredness and abdominal bloating had improved, but she still suffered from left jaw pain, which was only slightly relieved by dologesic. She also developed itchiness over both feet without associated rash. Other family members were also improving. One week later, her numbness had resolved and she only had mild jaw pain. There was no more diarrhoea or dizziness. Ciguatera poisoning Ciguatera poisoning is the most common fish-borne illness worldwide and one of the commonest form of nonbacterial food poisoning, with an estimated 10000 to 50000 people affected annually. In Hong Kong, the number of people affected in Year 2002, 2003 and 2004 were 60, 27 and 255 respectively.1 According to past records of ciguatera fish poisoning reported in Hong Kong, fish species which are more likely to contain ciguatoxins include Moray Eel (海鰻) , Lyretail Garoupa (石斑), Two-spot Red Snapper (紅曹), Humphead Wrasse (蘇眉), Tiger Garoupa (老虎斑), Flowery Garoupa (杉斑) and Spotted Coral Garoupa (西星斑).2 Ciguateric fish cannot be identified by appearance, taste, texture or smell. Quick and reliable screening tests for ciguateric fish poisoning are not yet available. In general, the larger the fish, the more likely and the higher the concentration of toxin present. Such fish are found in tropical waters, and so in Hong Kong, most of them are imported from areas such as the Nan Sha Islands and the South Pacific. Sizes of fish involved in reported cases usually ranged from one to five catties. Epidemiology Reaction occurs in up to 90% of ciguatoxin ingestions. Pathophysiology Ciguatoxin is a lipid-soluble polyether compound which is synthesised by specific bacteria after phagocytosis by the benthic dinoflagellate Gambierdiscus toxicus. The organism adheres to dead coral surfaces and bottom-associated algae. The toxin is then concentrated in the food chain. Ciguatoxin is a lipid-soluble polyether compound which is synthesised by specific bacteria after phagocytosis by the benthic dinoflagellate Gambierdiscus toxicus. The organism adheres to dead coral surfaces and bottom-associated algae. The toxin is then concentrated in the food chain. Multiple forms of ciguatoxin with minor molecular differences and pathogenicity were described. Ciguatoxin-1 (CTX-1) is the major toxin found in carnivorous fish and poses a human health risk at levels above 0.1 µg/kg fish.3 Symptoms (Table 1)4 Gastrointestinal symptoms often appear from the first day, lasting for one to two days. Neurological symptoms are usually multiple, varied, and can be bizarre. They begin within a few hours or up to three days after the meal, and can last several months. Cold sensation reversal is considered pathognomonic for ciguatera poisoning.4 Cardiopulmonary symptoms are uncommon, but can be severe.
Course Symptoms are noted within 6 to 12 hours after ingestion, but may begin within 15 minutes or be delayed until 24 hours after ingestion. Symptoms increase in frequency and severity over four to six hours, and last for 7 to 14 days. Some symptoms may take weeks or months to resolve. More severe cases usually have prior ciguatoxin exposure. Diagnosis The diagnosis is made clinically, although it may be supported by applying a validated mouse bioassay analysis and Cigua-Check analysis to the implicated fish by the Department of Health in Hong Kong.5 A coloured result means ciguatera is present; a clear result means the fish is safe to eat. Since there is no conclusive blood test for the presence of ciguatoxins, diagnosis depends upon the history and clinical features. Consumption of fish followed by an acute gastrointestinal and neurological illness is the usual clinical setting.
Management The general management is mainly supportive. There is no available antitoxin. Gastric lavage followed by activated charcoal might help if patients present with symptoms soon after ingestion. If the patient is suffering from gastrointestinal symptom, anti-emetics, anti-diarrhoeals, and intravenous rehydration can be considered. In case of symptomatic bradycardia, atropine can be used. Intravenous calcium gluconate may have some theoretical benefit in counteracting the inhibition of calcium uptake by excitable membranes. Amitriptyline has been shown to provide variable relief from neurological symptoms associated with ciguatera poisoning, e.g. pruritus or dysesthesias. The mechanism is perhaps by membrane stabilization via sodium channel blockade, or through its anti-cholinergic activity.6 An uncontrolled study using intravenous mannitol 0.5 to 1.0 g/kg in a 20% solution given over 10 to 30 minutes produced immediate resolution of symptoms in most of 24 patients so treated. The mechanism of action is unclear, but may be related to membrane stabilization.7 Prevention Prevention is of paramount importance. Family physicians have a major role. For suitable cases, we should seize the opportunities to promote preventive care. We can handle it in two ways. i) Purchase
ii) Consumption
Hon-ho Sze, MBBS (HK), FHKCFP, FRACGP
Medical Officer in-charge Tung Wah General Out-patient Clinic Wendy WS Tsui, MBChB (CUHK), FHKCFP, FRACGP, FHKAM (Fam Med) Associated Consultant Family Medicine and Primary Health Care, Hong Kong West Cluster, Hospital Authority Correspondence to : Dr Hon-ho Sze, Sai Ying Pun Jockey Club General Out-Patient Clinic, 134 Queen's Road West, Sai Ying Pun, Hong Kong SAR
References
|
|