|
September 2009, Volume 31, No. 3
|
Original Articles
|
The gender implications of sexual health education needs among Chinese early school leaversEleanor A Holroyd, William CW Wong 黃志威, Albert Lee 李大拔, Samuel YS Wong 黃仰山, Jonathan Wong, Phil WS Leung HK Pract 2009;31:120-127 Summary
Objective: The following paper examines the sexual health needs
of Chinese early school leavers from a gender perspective. The objectives were to
shed light on adolescent experience and their understanding of intimate relationships,
identify their knowledge of sex education and explore their sexual education needs.
Keywords: Sexual health, Chinese, adolescents, gender 摘要
目的: 本文從性別的角度研究華人過早退學者的性健康需 要,目的是闡述青少年對親密關係的體驗和理解,瞭解他們 所掌握的性教育知識及對性教育的需要。
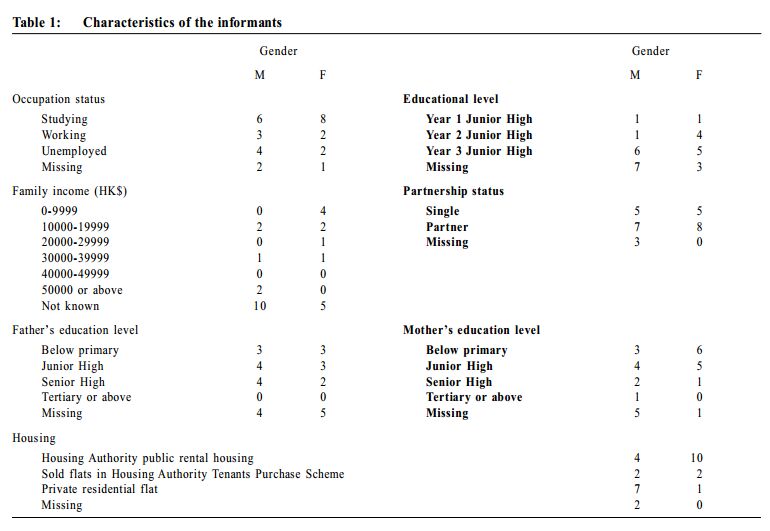
主要詞彙: 性健康,華人,青少年,性別。 Introduction Internationally there has been a steady decrease in the median age of the first sexual intercourse1 suggesting that the majority of young people begin sexual activity early in adolescence. The risk posed by unprotected sex is high with increasing rates of sexually transmitted infections (STI)2 and unwanted pregnancies in the Asia Pacific region including Australia. Swan et al's3 recent meta-analysis found that, in the United Kingdom, 55.4% of conceptions among under 16-year-olds ended in abortion. In addition, future suicide attempts have also been predicted following early sexual activity.4 In 2001 the annual Hong Kong Family Planning Association5 attendance figures for abortion almost doubled that of five years previously. In Hong Kong sexually experienced students (15-18 years old) reported poorer physical and psychological health as well as a diminished sense of well being.6 The tendency to treat such sexual risk-taking as an outcome of individual priorities is closely associated with the idea that sexual activity is based on a conscious choice; however, as Bourdieu states, "It is because agents never know completely what they are doing that what they do has more sense than they know".7 Sex education programmes that have targeted adolescents in the past have failed to delay the initiation of sexual activity, reduce the frequency, promote condom use or reduce the rate of teenage pregnancies.8-10 The lack of key elements such as a stringent gender specific perspective, a focus on knowledge and perception of STI/ HIV risks, identification of attitudes about sexual behaviour, promoting use of condom and advocating peer and adult communication about safer sexual practices, were identified as reasons for the failure of sex education programmes.9 Gender differences in adolescents' approaches to sexuality have received little attention in the literature. One area within the context of intimate relationships, showed that males tended to be more assertive than females when communicating about sex. 11-13 Evidence also suggests that young men and women differ in the strategies they use to communicate condom use.14 In Chinese society, adolescent males and females are also shown to differ in their abilities to negotiate sexual intercourse. 15 Effective sex education that controls and prevents HIV/AIDS is a regional and global health issue. It has been shown that social process es, characteristic of economies in transition, increase the likelihood of HIV/ AIDS outbreaks that Hong Kong and China are currently undergoing. Despite the many positive steps taken by governments in recent years towards controlling the epidemic, it is still growing fast at a time when the HIV/ AIDS epidemics in some neighbouring countries are stabilising. Gender-specific sexual health education programmes have alerted adolescents to the social and peer pressures that encourage negative sexual health behaviours. In places where these programmes have been implemented, lower proportions of male and female students commenced sexual activities.9 Correspondingly, pregnancy rates for females in the programme were lower as a result of both greater utilization of effective contraception and less sexual activity. In another study male students tended to evaluate formal sex education more positively and made greater improvements in sex education programmes than did females.16 A consensus exists that to be effective, sex education must encompass a range of contemporary adolescent cultural knowledge that differs with respect to aims, scope, implementation, and content in the programmes. 17,18 Little attention has been paid to the influence of gender and culture on such socially marginalized and hard to reach groups as "early school leavers". This group despite being at high risk of early sexual activities, are not serviced by formal health care systems. Adolescentsex education programmes in HongKong or internationally have been almost exclusively, school based programmes despite the fact that in 2001 approximately 34,000 adolescents (7.0%) aged 12-17 years old were not attending school.19 The little research that has been undertaken failed to take account of the settings in which adolescents live and or to elicit their perspectives. An understanding of the gender determinate of Chinese adolescent sexual activity and the corresponding targeting of appropriate interventions iscrucially important in terms of health promotion and policy development with the greatest need existing among those who have left the formal education system early. Methods The goals of the intervention study were to educate a group of adolescents to increase their knowledge and awareness of the factors involved in forming intimat e rel atio ns hips, p romo te po sitive attitudes to safer sex and improve their negotiation skills. It was intended that the findings would inform the development of a Chinese and gender-specific, multidisciplinary, sexual health programme targeting both out-of-school adolescents and the general public. The objectives for the sexual health needs assessment were to examine the influence of gender, adolescents' experiences of intimate relationships, their knowledge of sexual health education and their perceived needs for sexual health education. Subjects In Hong Kong ,the Young Men's Ch ristian Association (YMCA) caters for early school leavers through outreach social worker teams. Two branches of the YMCA, both of a similar geographic and demographic distribution, were selected as research sites. The sites were purposely selected as of lower socio-economic status and because of the high number of early school leavers in these districts who approached the YMCA. Early school leavers, for the purposes of this study, referred to youths aged 13-18 years who had left school or were highly irregular attendees (as defined by more time out of school than attending school over a subsequent school year). Evidence suggests that sex education should preferably start as close as possible to the onset of sexual activity.20-23 Twenty-eight adolescents were identified and interviewed by social workers from the two centres using convenience sampling and saturation theory (see Table 3). Each centre held four focus groups with members selected purposively by age and sex. Focus group discussions enabled in-depth interviews and allowed the researchers to obs erve wh en op inion shifted and un der what influences and circumstances. It also enabled more critical comments to be made by the adolescents24 when embarrassing topics such as sex were discussed.25,26 Four pilot interviews were conducted to ascertain the feasibility of the interview guide followed by modifications. Each focus group, conducted by a skilled moderator with an observer present, lasted approximately 1 hour and was tape recorded with the verbal consent of the members. Analysis Focus group data was analyzed according to the methods of inductive analysis involving concurrent data collection and analysis. Following each group discussion and individual interviews the audiotape was transcribed and translated into English where necessary. Each separate set of male and of female data was coded independently and compared, initially within the same sex groupings and then across both groups; inferences were drawn to explain similarities and differences in the findings. Translation of the data was undertaken by one researcher only to ensure consistency in interpretation. In addition, the translated data was checked by one member of the research team to ensure the translations accurately reflected the Chinese meaning. To ensure consistency and agreement in the coding of the data, data analysis was undertaken independently by two researchers. In addition, an audit trail was kept to ensure an accurate record of all decisions and processes undertaken during the study.27 Ethics Ethical approval was obtained from YMCA (Hong Kong) as well as the Chinese University Survey and Behavioral Research Subcommittee. Informed consent was obtained from each participant and anonymity and confidentiality were assured. Privacy during data collection and the right to withdraw at any time were also explained. Results In the demographic data, most of the girls (46.4%) and boys (53.6%) were within the 13 to 18-year-old age group (n=28); most claimed to be still studying and attending school on an irregular basis. (Table 1) Five boys (17.9%) and five girls (17.9%) were single at the time of interview and seven boys (25%) and eight girls (28.6%) said that they had a regular partner. Four boys (14.3%) and 10 girls (35.7%) lived in public housing estates, presumably with their families.
Comparing and contrasting gender based sexual health education needs A total of six gender-contrasting themes were found in the focus groups, these included: love and sexuality;the importance of appearance and body shape; feeling more positive after s ex; the need for separate sex education classes, preferred sources of health information and sexual health needs. The quotations and coding reference of informants attending focus groups are presented in Table 2.
Love and sexuality Some boys stated they were "okay" with visiting prostitutes and having one-night stands in direct contrast with the girls who believed that "love came before sex". Some boys stated that "sex " could make their relationships with a girlfriend closer. In contrast all the girls alluded to only wanting sex with the "one they loved". In respect to views about same sex relationships, more boys thought that homosexuality was "disgusting" than did the girls. The importance of appearance and body shape Appearance and body shape was strongly influential in forming relationships for the boys, with one boy stating that he appreciated the body of his girlfriend and another saying that 'good-looking' boys and girls would always attract others. Girls did not bring up this topic in the focus group discussions. "Feeling more positive after sex" The third theme was that of the link between sex and mood. The boys reported feeling more positive after sex, using such words as "happy", "excited", "comfortable" and "wanting more". In contrast, the girls felt afraid of getting pregnant or "played" on by their boyfriend. Sex education format The fourth theme was the degree of willingness to discuss intimate behaviours. Males s eemed more willing to discuss such matters as kissing, and sexual behaviours with friends than female informants. In respect to the teaching of sex education, more boys than girls thought that sex education classes should be co-educational, whereas more girls thoughts that such classes should be taught separately. More males thought that sex materials such as pornographic books/videos were normal or interesting (7 males), while more females rated these negatively using terms such as "abnormal" and "disgusting" (6 females). Preferred sources of health information The preferred sources of health information included the Internet (5 males), pornographic videos / books (2 males), social workers (2 females), and from science lessons (2 females). Sexual health education needs Both males and females stated that they needed more information about negotiating personal relationships and making friends. Finding the right person to teach sex education was seen as very important, for this specific group of young people. For example:
'I prefer to talk with a friend, since she is trust-able and have past (sexual) experience.'
(female) Although this population of boys and girls were interested in dating and appropriate sexual behaviour, they had little interest in being taught these issues formally. This perhaps highlights the lack of congruence between the emotional needs of adolescence and organizational agendas about risk reduction, sexual behaviour and the need for contraception. Both the boys and the girls highlighted the usefulness of small group, street based, education that was interactive and held in short sessions. For example,
'I prefer to learn in small groups, and each group should have at least one social
worker or teacher as leader, then our questions can be answered.' (male); Discussion In all interv iews, acro ss g ender and age, the importance of clarifying s ex roles and establishing sexual identity featured to differing extent. The girls' experience of sexuality may well have been systematically structured by pre-existing meanings and shaped by larger societal forces and constraints in the sense that sexual "choices" are systematic and sensible without being the outcome of premeditation and reflection. Therefore, the meanings and assumptions that currently define and inform young women's and young men's sexual lives and identities are often at odds with dominating moral values and sex education strategies preferred by education campaigns.28,29 In our study, female informants reported that identifying the social pressures exerted by friends and fear of pregnancy after sex had serious repercussion. A UK study reported that more females than males reported abstaining from sexual activity for fear of an unwanted pregnancy; instead of feeling uncomfortable, they felt that it was morally wrong, or felt uneasy or afraid of being taken advantage of. 30 For the girls interviewed value clarification, the links between love and sex and associated stigma were important as was addressing the disgust that they felt with pornography. It has been suggested that women are generally sexually motivated as an expression of love, while men are motivated by sex as a source of pleasure.31 The girls interviewed were less able to see sexual intercourse as a physical relationship without an emotional involvement than were the boys, highlighting differences between the sexes in respect of emotional involvement as a prerequisite for having sex. In a recent randomized controlled trial9 it was shown that girls' sexuality was associated with vulnerability by way of demands for s exual advances for unprotected s ex in a romantic relationship. The boys interviewed, in common with the girls, were either hesitant or too embarrassed to discuss sexual health with their parents and instead turned to informal sources such as the Internet (pornography) or popular teenage magazines. In concurrence with findings from a survey of secondary school sexual health needs recently conducted with junior high students in Hong Kong,32 the cultural reluctance to discuss sexuality and the fear of stigmatization, was a barrier to gaining formalized sex education for Chinese girls. In common with most other forms of everyday socialization, sexual interactions are not always deliberate or rationally calculated. The use of humour in the male group is one such example of providing a means to talk about sexuality and associated emotions.33 In contrast to the girls' expressions of worries and discomfort about sex without love, the boys joked about sex; emphasized the importance of confidentiality but did not elaborate on the nature of the personal information that may be confidential. The boys appeared to be reticent to voice their negative feelings and appeared confused about their personal responsibilities in sexual relationships. Both males and females highlighted the usefulness of the Internet, comics, small groups discussions and brainstorming as preferred means of sex education. Across cultures these latter activities have been shown to enable teenagers to personalize risks and be engaged in actively developing strategies and clear personal goals. 8,20 For these early school leavers, small groups and short programme interventions were seen to enable them to personalize risks and to be active engagement in developing clear personal goals. This study agrees with other research that suggests males tend to hold more permissive sexual attitudes, use more pornography and engage in more sexual encounters while employing a less emotional basis than do girls. However, little has been noted regarding the possible causes or implications of these findings. One possibility can be found in the recent writings of western feminists who emphasize that women 34-37 perceive the world in terms of relationships and closeness, whereas men attach more importance to individuality and are more impersonal. It is possible that these differences can be transferred to Chinese society in respect of implications for adolescent sex roles socialization and sex education. The focus group attendees of both sexes did not suggest that sex education encouraged their sexual experimentation or increased their sexual activity; in fact they were keen to learn from the "right" person. Conclusion Sexual health education currently provided in Hong Kong secondary schools needs to be reshaped to accommodate a more accessible and "youth friendly" reproductive health programmes and cross-sectoral interventions. More youth focused programmes that adopt a multidisciplinary approach while allowing sex segregation are needed. A gender specific approach that stresses competencies such as self-awareness, communication ,negotiation, and respect for and responsiveness to the opposite sex is also recommended. Implications for planning gender sensitive early school leaver outreach sex education
Acknowledgement We would like to express our sincere thanks to the Ho ng Ko ng SAR Go vernmen t's Health Care and Promotio n Fund , and all the informants for th eir collaboration.
Eleanor A Holroyd, BSc, PG Dip (Mid), PhD (Med. Anthro)
Professor of Asian and Gender Nursing, Head, Division of Nursing and Midwifery, School of Health Sciences, Bundora campus, RMIT University, Melbourne, Victoria, Australia William CW Wong, MD, MPH, FRCGP, FRACGP Associate Professor & Director of General Practice and Primary Care Education, Department of General Practice, University of Melbourne Albert Lee, MBBS, MPH, FHKAM (Fam Med) Professor & Director, Centre for Health Education and Health Promotion, School of Public Health, The Chinese University of Hong Kong Samuel Y S Wong, MD, MPH, FRACGP Associate Professor, Department of Community & Family Medicine, The Chinese University of Hong Kong Jonathan Wong, , BSSc AASECT Certified Sex Counselor, Rehabaid Centre, Hong Kong Phil WS Leung, MPhil Research Assistant, Department of Community and Family Medicine, The Chinese University of Hong Kong Correspondence to : Professor Eleanor A Holroyd, School of Health Sciences, Bundora campus, RMIT University, Melbourne, Victoria, Australia.
References
|
|