|
December 2011, Volume 33, No. 4
|
Case Report
|
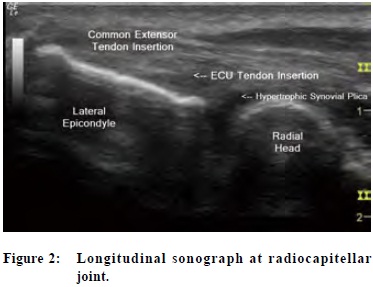
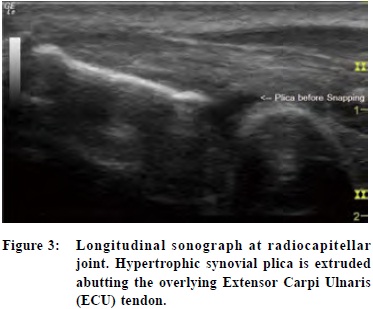
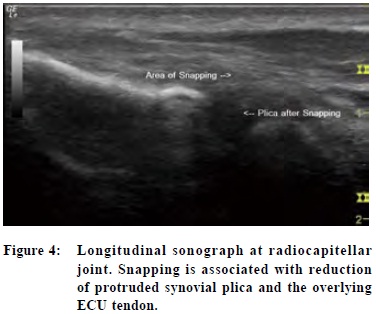
Snapping elbow syndrome: a report of two casesKeith K W Chan 陳國強, WK Wu 胡永強 HK Pract 2011;33:159-168 Summary Snapping elbow syndrome is an uncommon clinical entity with snapping occurring either at the medial or the lateral side of the elbow during certain motions of the elbow. Patients sometimes presents sometimes present with pain or local tenderness instead of snapping which may lead to the wrong diagnosis of the more common tennis or golfer's elbow syndrome. While making the clinical diagnosis of snapping elbow is obvious once the clinican is aware of the condition, to locate the cause of the snapping and arrive at an anatomical diagnosis can be difficult although it is crucial to successful treatment. In this article , we report two cases of snapping elbow syndrome, one at the lateral side and one at the medial side of the elbow, and share our experience with the use of musculoskeletal ultrasongraphy to arrive at an anatomical diagnosis of the condition. Keywords: Snapping elbow, medial, snapping elbow, lateral, musculoskeletal ultrasonography, ulnar nerve subluxation, medial head of triceps subluxation, synovial plica, real – time imaging, dynamic imaging 摘要 彈響手肘綜合症是一種不常見的病症,當手肘進行動作時,彈響會出現於手肘的內側或外側。但有些病人並無此典型病徵,只有痛楚或局部觸痛。因而易被誤診為較常見的網球手肘或哥爾夫球手肘綜合症。然而若能對這病症的存在保持警覺,診斷並不困難,但在判斷其成因和在解剖學上病變的位置時,則並不容易。而這些資料對於成功治療是很重要的。本文報告了兩個彈響手肘案例。一個發生在手肘外側及另一個在內則,並詳述我們在使用肌肉骨骼超聲波檢查作解剖學上診斷的經驗。 主要詞彙: 彈響手肘,內側,彈響手肘,外側,肌肉骨骼超聲波檢查,尺神經半脫位,肱三頭肌內側頭半脫位,滑膜皺襞,即時成像,動態成像 Introduction Snapping elbow is a dynamic phenomenon where a snapping is a visible palpable or audible during elbow joint movement, the condition is uncommon and generally poorly understood by clinicians. It may be associated with pain 1 which makes it easily misdiagnosed as other commonly encountered elbow conditions including tennis elbow or golfer's elbow syndrome. Once the snapping is recognized, further structural pathology of the snapping structures should be sought because precise anatomical diagnoses determine potential for successful treatment. For example, studies showed that ulnar nerve transposition surgery would fail with persistence of symptoms if the associated snapping medial head of tricepts was unrecognized and not property treated at the same time.2,3 To make an anatomical diagnosis of snapping elbow, ultrasonography and magnetic resonance imaging (MRI) are usually advocated as investigation tools before arthroscopy. The purpose of this article is to report two cases of snapping elbow syndrome with a description of their diagnostic process and to review such clinical entity with relevant literature. Materials and methods We studied two male patients with the complaints of snapping elbows (one at the lateral side and one at the medial side). Both patients were assessed by the authors and the snapping was confirmed clinically by history taking and physical examination.Musculoskeletal ultrasonographic studies were then performed by the authors, both of whom received prior relevant ultrasonography training. A phased array linear 12L-RS transducer (LOGIQ-e, GE Ultrasound, USA) was used. Case 1 Patient LWK, a 52-year-old male right-handed manual worker, presented to the author's clinic with a painful lateral right elbow associated with snapping at his lateral right elbow region during elbow region during elbow motions. The pain was localized without radiation. He reported that his problems started insidiously about 6 months ago after some weight lifting jobs. There was no history of overt sprain or contusion over his right elbow at that time or in the past. The pain was gradually increasing in severity and sometimes prevented him from prolonged weight lifting. Occasionally, sudden pain with snapping during elbow motions would cause his arm to give way. He denied associated numbness, tingling, burning or paresthesia over his right elbow and arm. He did not have any other complaints over his left elbow. Physical examination of his right elbow revealed no cubitus deformity and no erythema or swelling around the elbow. Palpation elicited tenderness at the radiocapitellar joint line, over the common wrist extensor tendon near its insertion. The right elbow's range of motion (ROM) was full in all directions. By actively or passively flexing and extending the pronated elbow back and forth, a visible snap was notices over the lateral elbow at an angle of around 80-90 (Video Clip 1).4 No associated clicking or locking could be demonstrated. Further clinical examination showed no ligamentous laxity or joint instability over the lateral elbow. The clinical diagnosis was snapping lateral elbow. The offending structure could be a hypertrophic synovial plica, but a torn annular ligament could not be ruled out. The parient then underwent a musculoskeletal ultrasonogrpahy of his right elbow to delineate the pathology (Figure 1). Sonographic findings of patient LWK demonstrated that the snapping of his right elbow occurred at the lateral elbow occurred at the lateral elbowbetween the capitellum and the radial head in long axis view (Figure 2). The snapping structure involved was a hypoechoeic structure (Figure 3) which extruded gradually from the radiocapitellar joint when the elbow was flexed, pushing the extensor carpi ulnaris (ECU) to flip with an associated snapping (Figure 4, Video clip 2).5 This most likely represented a posterolateral hypertrophic synovial plica at the radiocapitellar joint.
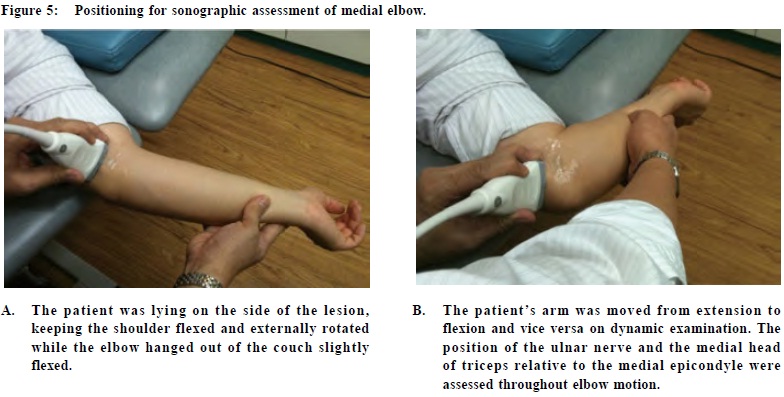
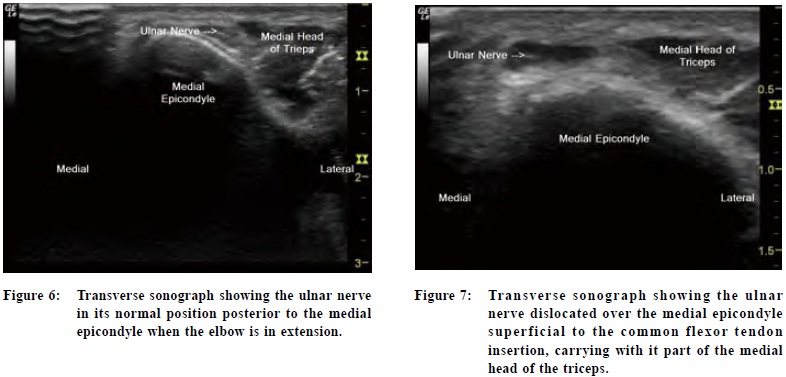
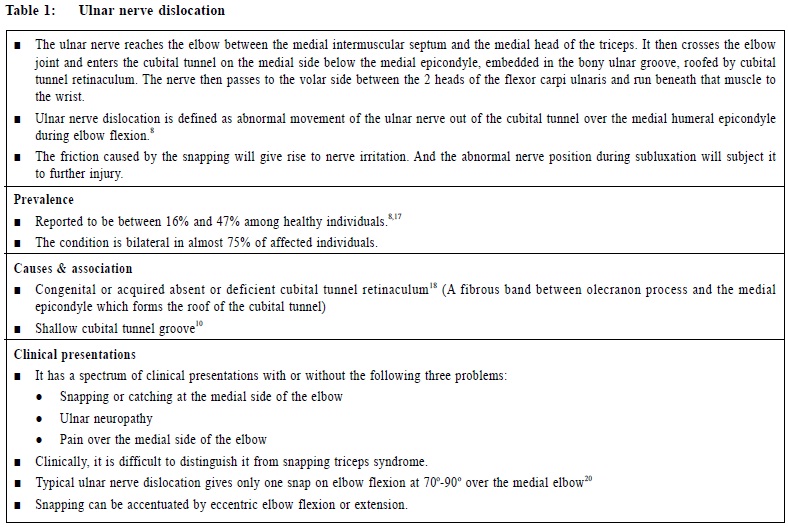
Case 2 Patient NLF, a 23-year-old male right handed clerk, presented with snapping over his medial left elbow during motion. The patient had a sprain injury to his left elbow 2 years ago when he accidentally gave way during an overhead weight lifting exercise. Immediately after the injury, he experienced pain and swelling at inflammation, he started to notice snapping at the medial side of his elbow during elbow flexion and extension. The snapping was sometimes associated with mild tingling sensation at the ulnar side of his forearm and hand. The physical examination of his left elbow revealed no cubitus deformity and no edema or erythema around the elbow. Palpation did not elicittenderness but revealed snapping on the medial elbow during flexion and extension to around 80. The snapping was accentuated on resisted elbow flexion.Active and passive ROM of the left elbow was full in all directions. No associated clicking or locking could be demonstrated. Further clinical examination showed positive ulnar Tinel's sign at the cubital tunnel. When the elbow was passively flexed and extended, the ulnar nerve could be felt dislocating from its groove (cubital tunnel) at the posterior aspect of the humeral epicondyle during elbow flexion. Otherwise, no ligamentous laxity or joint instability could be found. The clinical diagnosis was snapping medial elbow caused by the ulnar nerve subluxating out of its cubital tunnel during flexion. A musculoskeletal ultrasonography of his left elbow was then arranged to confirm the pathology of the snapping structure(Figure 5). Sonographic examination demonstrated that the ulnar nerve was in the cubital tunnel when the elbow was fully extended (Figure 6). On elbow flexion, the ulnar nerve subluxed over the medial epicondyle carrying with it part of the medial head of the triceps (Figure 7). When the elbow returned from flexion to extension, the ulnar nerve reduced back to the cubital tunnel over the tip of medial epicondyle. Such reduction was associated with a visible snapping on the screen (Video Clip 3).6 The sonographic diagnosis was ulnar nerve dislocation with subluxation of the medial head of triceps. The diagnosis was later confirmed by findings at surgery (Figure 8, Video clip 4).7
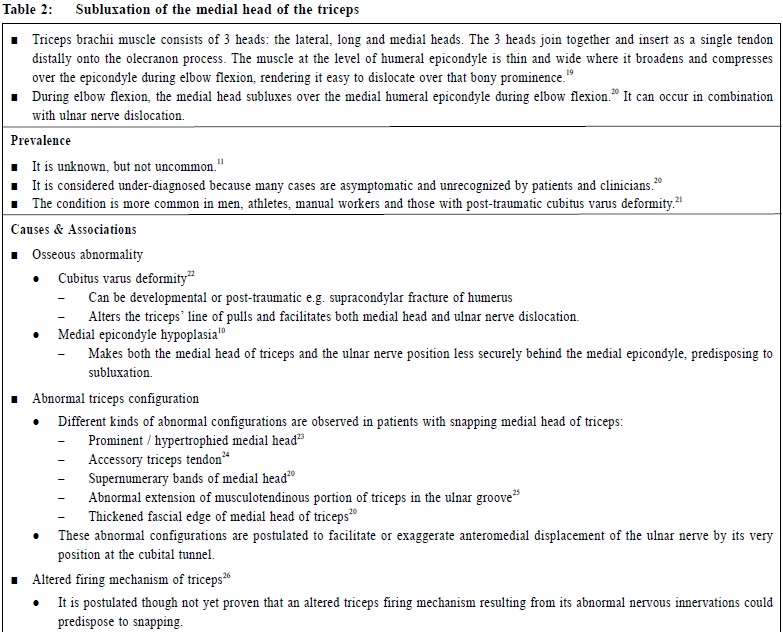
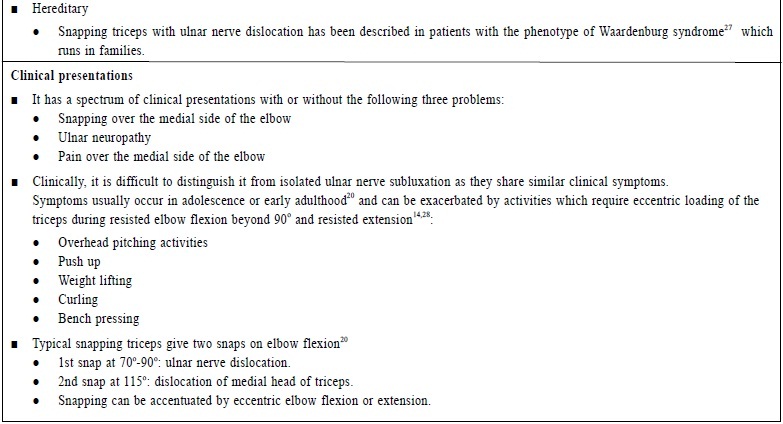
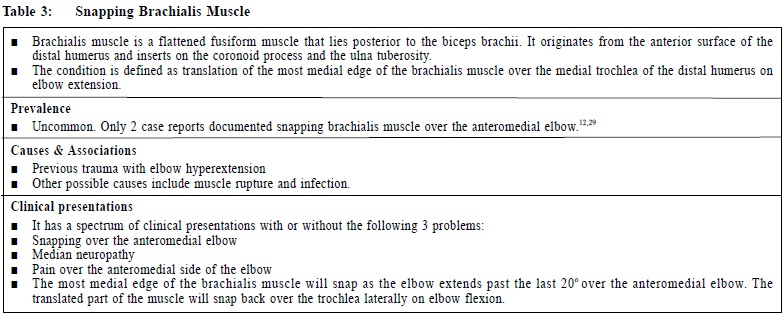
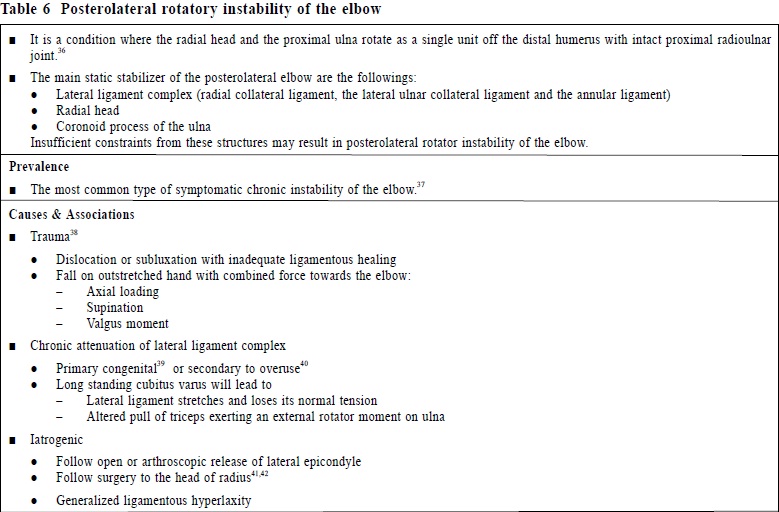
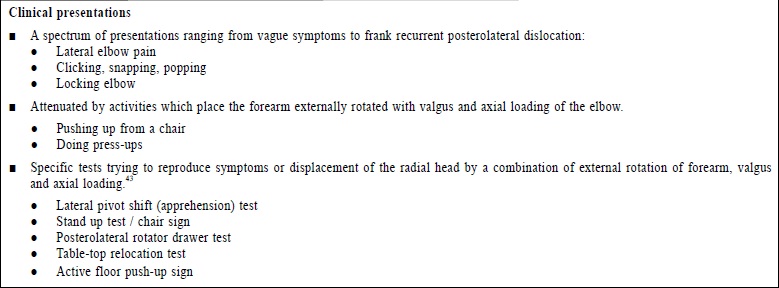
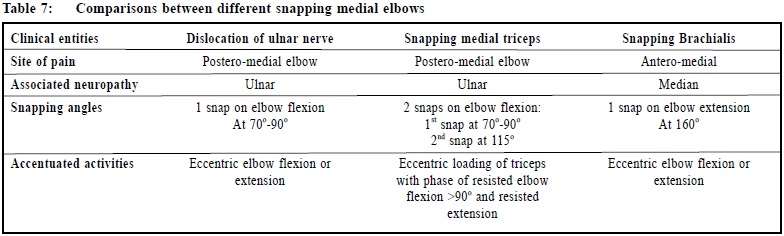
Discussion In 1970s, the terms "snapping elbow" has been regarded synonymous to slipping of the ulnar nerve out of the cubital tunnel during elbow flexion.8 Reports in recent several decades identified some other structures or conditions that can contribute to snapping over the elbow. Extra-articular causes include ulnar nerve dislocation with or without associated subluxation of the medial head of the triceps 9,10,11, and snapping brachialis muscle.12 Intra-articular causes include intra-articular loose bodies 13, hypertrophic synovial plica impingement at radio-humeral joint 14-16 and torn annular ligament.15-16 Other possible causes include tumors, previous surgery or trauma, articular degeneration and inflammatory processes. This case report demonstrated a case of medial snapping elbow caused by ulnar nerve dislocation associated with subluxation of the medial head of the triceps. It is one of the commonest causes of snapping elbow syndrome. Three differential diagnoses for MEDIAL SNAPPING ELBOW are commonly quoted from literature:
1. Ulnar nerve dislocation (Table 1)
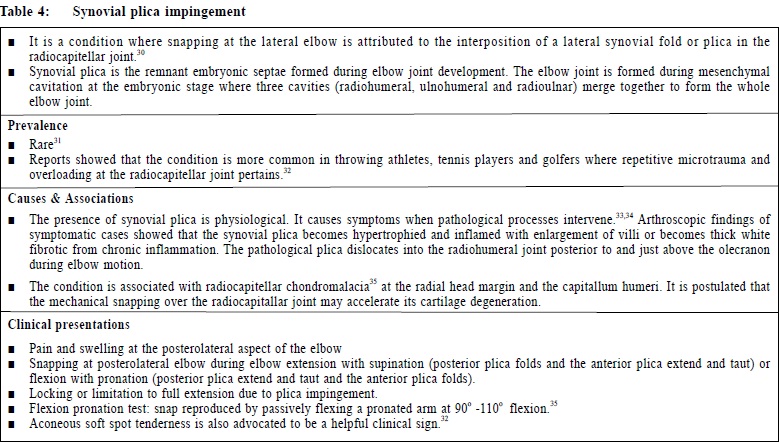
From literature, snapping elbows are most frequently related to medial anatomical structures. Here, we also presented a case of lateral snapping elbow, where the ECU tendon flicked over the hypertrophic synovial plica from the radiocapitellar joint, resulting in snapping. Serveral recent reports brought LATERAL SNAPPING ELBOW into the spotlight. Differential diagnoses include:
1. Synovial plica impingement (Table 4) To approach a patient with snappin gelbow, a detailed pain history of how and when the snappings occur would give hints on the cause of the snapping. Once the snapping phenomenon is clincially determined, its anatomical diagnoses should then be sought as it is crucial for successful treatment. Our case studies have demonstrated that musculoskeletal ultrasonography is a powerful tool for making the anatomical diagnoses. Since the snapping elbow syndrome is a dynamic phenomenon, musculoskeletal ultrasonography has the advantage of real-time imaging as physicians can put the patients' elbows in motion to reproduce the snapping and focus on that particular region inder real-time scanning . to find out the causative structure or mechanism. MRI on the other hand has an inherent Limitation as a static cross-sectional examination and therefore may be difficult in assessing the transient snapping phenomenon. The limitations of this study include the limited number of subjects as snapping elbow syndrome is in general uncommon. In case 2, the sonographic diagnosis was finally confirmed by intra-operative findings. Howeverm as the case 1 paritent refused sugery, the sonographic diagnosis could not be confirmed operatively but the sonographic findings of that case were further verified by one of the world experts in musculoskeletal ultrasongraph to ensure accuracy. Conclusions This artical highlights 2 cases of snapping elbow synfrome, one snapping on the lateral side from hypertrophic synoivial plica abutting on ECU, another one snapping on the medial side from dislocation of ulnar nerve with subluxation of medial head of triceps. Upon clinical examination of the elbow, snappin gwas evident in both cases but the precise snapping structures could not be confidently delineated clinically . Musculoskeletal ultrasonography was able to display realtime images of the causative snapping structure(s) disputing that they are transient when the elbows were put into motion. It is consifered that musculoskeletal ultrasonography can be the investigation of choice to evluate snapping elbow syndrome. Acknowledgements I wish to thank Thomas B Clark, DC, RVT, an internationally renowned expert in musculoskeletal ultrasonography for his help in verifying sonographic findings of the presented cases. I also wish to thank Dr Yeung Sai Hung, a specialist in Orthopedics and Traumatology, for preparing intro-operative photos and video clips of Case 2.
Keith KW Chan, MMPhysMed (Mu.sk)(Syd), FHKAM(FM), FRCGP(UK), FRACGP
Ricky WK Wu, PGDipMSM (Otago), FHKAM(FM), FRACGP, FHKCFP Musculoskeletal Physicians and Specialists in Family Medicine
Correspondence to : Dr Keith KW Chan, The Hong Kong Institute of Musculoskeletal
Medicine, Room 1201, 12/F, City Landmark I, 68 Chung On
Street, Tsuen Wan, Hong Kong SAR.
References
|
|