|
March 2013, Volume 35, No. 1
|
Original Articles
|
Ambulatory blood pressure monitoring (ABPM) for hypertension management in primary care setting: an experience sharing from Kwong Wah HospitalLap-kin Chiang 蔣立建, Lorna Ng 吳蓮蓮 HK Pract 2013;35:5-11 Summary
Objective: To study the indications for ambulatory blood pressure
mon i tor i ng (ABPM) ordered by primary care physicians, and to assess its effects
on hypertension management.
Keywords: Ambulatory blood pressure monitoring, hypertension, primary health care 摘要
目的: 評估基層醫療醫生安排動態血壓監測的適應症和監測對高血壓治療的影響。
主要詞彙: 動態血壓監測,高血壓,基層醫療 Introduction Hypertension remains a key risk factor for cardiovascular diseases. It is also the largest cause of morbidity and mortality worldwide, yet only about half of patients on treatment have their blood pressure (BP) controlled to current recommended levels.1,2 The Population Health Survey 2003-04 revealed that 27% of the Hong Kong population aged 15 or above had increased blood pressure.3 Clinic BP measurements exhibit enormous variability, which hinders accurate classification and frustrates both health service providers and patients.4 Ambulatory blood pressure measurement (ABPM) is a non-invasive, fully automated technique in which BP is recorded over an extended period of time, typically 24 hours.5 ABPM provides practising physicians with a more comprehensive perspective on blood pressure management than might be available from office (or casual) blood pressure measurements. It improves the detection rate for clinically significant blood pressure changes that may go undetected during a brief daytime visit to the physician's office.6,7 ABPM has been shown to be superior to office measurements for predicting hypertensive target organ damage.8,9 Ordering of ambulatory blood pressure monitoring (ABPM) in Family Medicine and General Outpatient Department of Kwong Wah Hospital increased dramatically from 11 cases in year 2008 to 119 cases in year 2011. However, the reasons why physicians requested ABPM and the effects of ABPM on clinical hypertension management remained unknown. Objectives
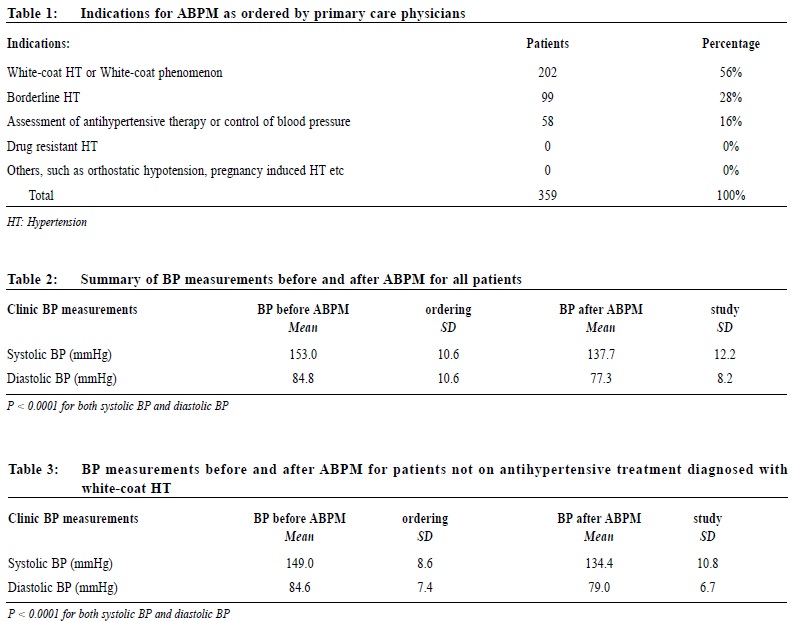
1. To delineate the reasons why primary care physicians request ABPM; Methodology This is a retrospective review study. Medical records of all patients who had received ambulatory blood pressure monitoring (ABPM) in the Family Medicine and General Outpatient Department of Kwong Wah Hospital from January 2008 to June 2012 were traced and reviewed. Physician's indications for ABPM were categorized according to the American Academy of Family Physicians' (AAFP) recommendation.10 Changes in management of hypertension and levels of blood pressure control analyzed after ABPM were made. (See: Appendix 1 - Flowchart of Study). The blood pressure measured on the day of ABPM ordering and preceding medical attendance were traced and averaged. The averaged BP reading was termed as "before ABPM BP". The blood pressures measured on the subsequent consecutive two follow-up attendances after review of ABPM report were traced and averaged as "post ABPM BP". The follow-up interval was usually around 5 to 7 weeks. Student's t-test was used to examine the mean blood pressure difference before and after ABPM. All analyses were conducted using the Statistical Package for the Social Sciences version 19 (SPSS Inc., United States). ABPM device and report All ABPM were performed by the Cardiac Unit at Kwong Wah Hospital. The device (Accutracker Dx, SunTech Medical Instruments) was programmed to record blood pressure and heart rate at 30-minute intervals. Standardized reports were verified by authorized doctors from the Cardiac Unit, which included patient demographic data, average, awake and asleep blood pressure, blood pressure load, average heart rates and customized blood pressure and heart rate graphs. Definitions Sustained hypertension was defined as a systolic blood pressure ≥ 135/85 and ≥ 120/75 mmHg in day-time and night-time respectively. White coat hypertension was defined as a blood pressure ≥140/90 mmHg when measured in office or clinic setting, and < 135/85 mmHg during 24-hour ABPM.10,11 Results 379 ABPM were performed from January 2008 to June 2012. Of these, 20 cases were excluded for analysis because of incomplete data. 133 males and 226 females patients were included for analysis. Their mean (SD) age were 61.8 (14.3) and 61.8 (11.4) years respectively. 59% were on antihypertensive treatment at day of ABPM ordering. 70.8% (254/359) had at least one chronic disease, which included hypertension, diabetes mellitus, hyperlipidaemia, chronic renal impairment, coronary heart disease or stroke. The indications for ordering ABPM were summarized in Table 1, with 56% (202/359) for "white-coat hypertension" or "white-coat phenomenon", 28% (99/359) for patients with "borderline hypertension", and 16% (58/359) of patients for "assessment of antihypertensive therapy or control of blood pressure". After ABPM, 50.1% had a change in their antihypertensive therapy. Among patients who were not on antihypertensive treatment before ABPM, 18% (64/359) were confirmed by ABPM to have whitecoat hypertension. Among those patients who had been on antihypertensive treatment before ABPM, 30% (107/359) were confirmed by ABPM to have white-coat phenomenon. Before ABPM, the mean (SD) of systolic blood pressure (SBP) and diastolic blood pressure (SBP) of all patients recorded were 153.0 (10.6) and 84.8 (10.6) mmHg respectively. On the subsequent followups after review of the ABPM report and relevant adjustment of hypertension treatment, the mean (SD) of SBP and DBP recorded were 137.7 (12.2) and 77.3 (8.2) mmHg respectively (Summarized in Table 2). Among the white-coat hypertension and other patients who did not receive any antihypertensive medication, 21 male and 43 female patients were confirmed to have white-coat hypertension. The mean (SD) systolic blood pressure (SBP) and diastolic blood pressure (DBP) before ABPM were 149.0 (8.6) and 84.6 (7.4) mmHg respectively (Summarized in Table 3). The mean (SD) SBP and DBP were 134.4 (10.8) and 79.0 (6.7) mmHg respectively on the subsequent follow up (P < 0.0001 for both SBP and DBP). Among those patients who were on antihypertensive treatment before ABPM, 41 male and 66 female patients were confirmed to have white-coat phenomenon. This group of patients however did not receive any adjustment in their antihypertensive treatment following ABPM reviewing. As shown in Table 4, the mean (SD) SBP and DBP before ABPM was 151.7 (9.4) and 83.4 (13.7) mmHg respectively. The post ABPM BP level was significantly lower, with mean (SD) of SBP 138.4 (11.8) mmHg and DBP 75.7 (8.5) mmHg respectively (P < 0.0001 for both SBP and DBP). Discussion No patient was referred for ABPM for drug-resistant hypertension, pregnancy-induced hypertension, orthostatic hypotension or evaluation for suspected autonomic dysfunction. This is likely to be because these patients have already been referred to hospital specialist clinics for further management. As shown in Table 1, the indications for ABPM were in accordance with the AAFP recommendations. ABPM appears to have a positive effect on hypertension management. Firstly, ABPM helped referring physician to confirm patients' diagnosis, especially in making the diagnosis of white-coat hypertension. ABPM also provided primary care physicians with more data for making changes in antihypertensive therapy. Diagnostic or therapeutic challenges can be solved with results from ABPM helping physicians in their decision-making process.5 After ABPM, 50.1% of patients had changes made in their antihypertensive therapy. The hypertension control for all patients was significantly improved on subsequent follow-up. Grin JM also reported similar finding in their study.5 It is speculated that improved blood pressure control in those patients could yield reduced target organ involvement or hypertension related complications.8
White-coat hypertension Studies suggest that 15 to 30 percent of patients who were hypertensive in the clinic setting were normotensive at other times.7,11 According to the Tam et al's study conducted in Hong Kong, which recruited patients in the primary care clinic of Department of Health, the percentage of white-coat hypertension (WCH) in their study population was 28.2%.12 In our study, 18% patients were confirmed to have WCH, which was lower than that in Tam et al's study. The reason for our WCH patient number was lower might be that some of our patients, confirmed to have WCH, did not have subsequent follow-up blood pressure measurements, and therefore they were excluded from the study. Our study also found that 30% of hypertensive patients already on antihypertensive treatment had white-coat phenomenon. Recognition and proper management of these subgroups would allow a reduction in antihypertensive medication use and a decrease in related side effects.10 It is generally accepted that patients with white-coat hypertension are at relatively low risk of cardiovascular diseases and are unlikely to benefit from antihypertensive drug treatment.13 With the availability of ABPM data to confirm white-coat hypertension, primary care physicians of our department are confident in withholding antihypertensive drug treatment, and therefore avoiding side effects, such as hypotension caused by drug treatment. Similar finding was reported in Grin JM's study,5 physicians in both private and hospital practice indicated they felt confident in the treatment decision after 24-hour ambulatory monitoring. As shown in Table 3, the mean BP for this subgroup of patients was normal on the subsequent follow-up. However, it is not clear why those patients' BPs on subsequent follow-up even in clinic setting became normal. It is probable that they were less anxious after knowing that they were not suffering from hypertension. In the face of a diagnostic challenge as posed by the high prevalence of WCH among our hypertensive patients, ABPM would play an essential role in establishing the diagnosis of hypertension firmly before implementation of anti-hypertensive therapy.4 Nearly one fifth of the patients with elevated blood pressure in clinic setting might have been treated for hypertension if the possibility of WCH was overlooked by the case physician. Consequently, this might lead to a substantial number of patients suffering from medication side effects. This study illustrated that both white - coat hypertension and white-coat phenomenon were common in the primary care setting. Primary care doctors should be more careful and should consider arrangement of ABPM while considering to start or adjust drug therapy for those patients suspected to have white-coat hypertension or have white-coat phenomenon. Limitations The study is a retrospective review study, which did not include controls. Therefore, it is difficult to conclude that improvement on hypertension control is directly related to ABPM. While the general outcome in our patient population at the Kwong Wah Hospital has been rewarding, it is uncertain whether these findings can be extended to the general population of hypertensive patients. However, our findings might stimulate investigators to conduct well designed study to examine whether ABPM changes the outcomes of hypertensive care. Conclusion The ordering indications of ABPM at our Kwong Wah Hospital are in accordance with American Academy of Family Physicians recommendation. Both of whitecoat hypertension and white-coat phenomenon are common in primary care setting. With the availability of ABPM results and making relevant adjustment in hypertension management, blood pressure control is significantly improved.
Lap-kin Chiang, MBChB (CUHK), MFM (Monash)
Resident Lorna Ng, LMCHK, MPH (CUHK), FHKCFP, FHKAM (Fam Med) Senior Medical Officer i/c Family Medicine and General Outpatient Department, Kwong Wah Hospital Correspondence to : Dr Lap-kin Chiang, Family Medicine & General Out-patient Department, 1/F, Tsui Tsin Tong Outpatient Building, Kwong Wah Hospital, 25 Waterloo Road, Mongkok, Kowloon, Hong Kong SAR.
References
|
|