|
June 2021,Volume 43, No.2
|
Original Article
|
Prevalence of urinary incontinence in Chinese elderly male in primary care setting and their quality of life in Hong KongWan-ying Tse 謝韻盈,Damian CH Siu 蕭志康,Chi-keung Yeung 楊志強,Kin-wing Chung 鍾建榮,Shuk-yun Leung 梁淑茵,Eric MT Hui 許明通 HK Pract 2021;43:35-45 Summary
Objective:
To study the prevalence of urinary
incontinence in Chinese elderly male in primary care
and its effect on their quality of life.
The quality of life measured by KHQ was worse when the severity of urinary incontinence increases. Conclusions: Urinary incontinence is common in Chinese elderly males and has a negative impact on their quality of life. Benign prostatic hyperplasia was significantly associated with urinary incontinence.Keywords: Urinary incontinence, elderly, ICIQ-UI SF, King’s Health Questionnaire, epidemiology. 摘要
目 標 :
研究基層醫療中老年男士尿失禁的發病率以及其
對生活質量的影響。
主要詞彙 : 尿失禁,老人,國際失禁問卷-尿失禁簡表, 金氏健康問卷,流行病學。 IntroductionBackground and objectives Urinary incontinence is defined by the International Continence Society (ICS) as the involuntary leakage of urine.1 It is a common medical condition that affects up to 55% of female and 34% of the elderly male population according to studies conducted in the United States.2-3 In Hong Kong, it was found that 49.1% of female was found to have urinary incontinence in the primary care setting.4 Yet no local data is available for male urinary incontinence in primary care. Urinary incontinence is at least twice as common in women than in men.5 As a result, a large number of studies have been focused on female urinary incontinence while studies addressing the problem of male urinary incontinence and its impact on their quality of life are scarce.5-6 Results from epidemiologic studies show that male incontinence is a relatively uncommon problem in young men but there is a precipitous rise in its prevalence with increasing age.5,7-8 Although not life- threatening by itself, urinary incontinence in male is bothersome and has deleterious effects on a person’s quality of life, such as physical health, psychological well-being, and sexual satisfaction.9-10 Despite these negative impacts, patients often do not volunteer this problem to the healthcare professionals.9,11 In addition, male urinary incontinence poses a great financial burden to society. It was estimated that 3 billion dollars were spent on managing male urinary incontinence and its complications in the United States in the year of 2000.12 Some of the causes of male urinary incontinence, such as urinary tract infection, overactive bladder, faecal impaction, and diabetes are amenable to medical therapies.11,13-14 Being the first point of contact in the healthcare system, family physicians are in an ideal position to screen for urinary incontinence and manage the condition via administering treatment or referring the patient to the appropriate secondary center.11,14-15 Such increase in sensitivity in the detection and prompt treatment or amelioration of urinary incontinence would potentially result in a substantial lowering of the healthcare cost and marked improvement in the patients’ quality of life. Given the huge implications of urinary incontinence, it is important for primary care physicians to heighten their awareness in the recognition of such a medical issue. In fact, in the 2017 HK Reference Framework for Preventive Care for Older Adults in Primary Care Settings, it is recommended that opportunistic screening for urinary incontinence should be done for the elderlies.16 However, no local data regarding the prevalence of urinary incontinence in elderly male in the primary care setting is available to lend further support to such recommendations. Prior to the 1990s, the reported prevalence of urinary incontinence varies greatly across different studies, which was attributed in part to the lack of a universal tool in the assessment of urinary incontinence.5 This problem was subsequently resolved by the development of the International Consultation on Incontinence Questionnaire Short Form (ICIQ-UI SF) by the International Continence Society. The ICIQ-UI SF is a validated questionnaire which assesses the presence and severity of urinary incontinence and is available in various translated languages. It provides a standardised method and unifying platform that facilitates researchers around the globe in the evaluation, comparison, and discussion of urinary incontinence.17-18 Only 2 epidemiological studies using the ICIQ-UI SF have been conducted on male urinary incontinence up to date, with a reported prevalence rate of 14.8% and 14.2% in Australia and Brazil respectively.19-20 The primary objective of this study was to determine the prevalence of urinary incontinence as no local data was available, the associated risk factors and its effect on the quality of life of elderly male patients in the primary care setting using the ICIQ-UI SF and King’s health questionnaire. Such data would help the healthcare professionals to gauge the severity of this problem in the local community and allow healthcare providers to suggest recommendations on management, professional training, and public education programs. MethodologyStudy designThis was a cross-sectional pilot study. Subjects were recruited from Fanling Family Medicine center in Hong Kong from 1st to 31st March 2018. Inclusion criteria were Chinese male at 65 years old or above. Exclusion criteria included non-Chinese men, and those who were unable to consent to the study. Sample size was calculated as 330, to accept an absolute sample error rate of 5% at 95% confidence level. The expected proportion in population was set to be 0.15 from previous urinary incontinence prevalence studies in male (Australia 0.148, Brazil 0.142, Taiwan 0.15).19-20, 27
Sample size was calculated
by the sample size formula: Assuming the response rate was 60%, we calculated a sample size of 196/0.6 = 326 individuals, which would round up to 330. We would therefore aim at recruiting at least 330 individuals. MeasurementsThe ICIQ-UI SF (International Consultation on Incontinence Questionnaire Short Form) was developed by the International Continence Society, in an effort to produce internationally applicable questionnaire for clinical use and research. It consists of four questions assessing the frequency, amount, types of urinary incontinence and the impact on the quality of life in the past 4 weeks. It has been validated and translated into different languages. It has been used in various studies across different countries.17-18 The Chinese Version of ICIQ-UI SF is readily available and has been validated by Shiow-ru Chang et al21 and Liang Huang et al.22 The ICIQ-UI SF has a score ranging from 0-21. There is currently no consensus on the interpretation of ICIQ-UI SF, and we adopt the interpretation described by Klovning A et al, that patient is defined to have incontinence with a score of 1 or higher, with higher score indicating more severe urinary incontinence. The score can be further classified to slight (1-5), moderate (6-12), severe (13-18) and very severe (19-21) urinary incontinence.23 The King’s health Questionnaire is a validated quality of life questionnaire that was initially developed to assess the health impact on urinary incontinence in female.24 It was subsequently shown that the questionnaire is also reliable and valid for the assessment of quality of life in male urinary incontinence.25The questionnaire consists of 21 questions, representing assessment of different domains including general health perception, incontinence impact, role limitations, physical limitations, social limitations, personal relationships, emotions, sleep and energy, and severity measures. The questions were converted to a score ranging from 0 to 100, and a higher score indicating that the quality of life is more negatively affected. Data collectionWe collected the data using a printout questionnaire, consisting of three parts: 1) Demographics, including age, marital status and educational status, past medical and surgical history such as types of chronic illnesses and any previous history of prostatic surgery; 2) The score of the Chinese version of ICIQ-UI SF; and 3) The score of Chinese version of King’s Health Questionnaire. Patients were asked to complete part 3 (The King’s Health questionnaire) when urinary incontinence has been reported in part 2 (i.e. ICIQ-UI SF score ≥1). (See Appendix) Questionnaires were distributed by clerical staff to patients attending consultations consecutively in a general outpatient clinic who met the inclusion criteria (Figure 1). Information sheets about the study were given. Patients were then interviewed by the principal investigator or a trained intern, in an attempt to complete the questionnaires. 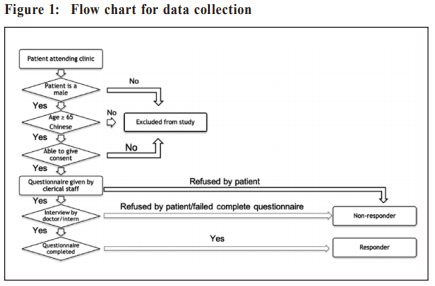 Patients who refused to participate or give consent in the survey and those incomplete questionnaires were regarded as non-responders. Ethical considerationsInformed consent in written form was obtained from all patients. The study was approved by the New Territories East Cluster - Chinese University of Hong Kong (NETC-CUHK) clinical research ethics committee (CREC Ref. No: 2017.655) and the North District Hospital, NTEC Ethics committee. Patients were managed according to the Declaration of Helsinki.
Outcomes
Statistical methods
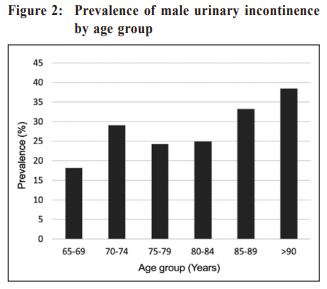
The independent variable was urinary incontinence scored by the ICIQ-UI SF form, and the dependent variable was the quality of life score by the King's Health Questionnaire. The relationship between independent and dependent variables was analysed using Spearman’s Correlation Coefficient. Findings were considered statistically significant when p < 0.05. The relationship between severity of ICIQ-UI SF score and different age categories was tested using one-way ANOVA. Binary logistic regression was used to identify features associated with urinary incontinence. ResultWe distributed 444 questionnaires, twenty-seven patients refused to participate in the study, while 1 questionnaire was incomplete. A total of 416 subjects was therefore recruited with a response rate of 93.7%. The demographics of the subjects were shown in table 1. The mean age of continent and incontinent men was 74.44 (CI 73.01-75.86, SE 0.718) and 72.87 (CI: 72.12- 73.63, SE: 0.382) respectively. One hundred and one patients reported to have urinary incontinence (i.e. ICIQ-UI SF score >1), corresponding to a prevalence rate of 24.3%. The prevalence increased as patient’s age increased (Table 1).  The mean score of ICIQ-UI SF was 6.57 ± 2.762 (SD). The highest score in our subject was 16. The ICIQ-UI SF score was further categorised according to the level of severity (Table 2). 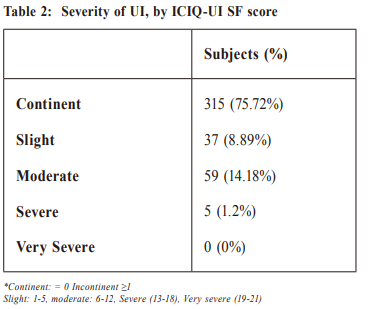 One-way ANOVA was used to assess the ICIQ- UI SF score of different age groups among incontinent men. There was no significant variation in the score among different age groups of incontinent male UI, with F (5, 95)=0.435, p=0.823, r=0.0675. The most common type of urinary incontinence was urge incontinence (57.4%), followed by mixed incontinence (23.8%), post micturition dribbling (11.9%) and stress incontinence (4%). Four percent of our patients leaked without obvious reason and 1% of patients leaked all the time. Only benign prostatic hyperplasia (BPH) was identified as a significant risk factor to male urinary incontinence as shown by binary logistic regression. The unadjusted and adjusted OR were 1.995 (CI 1.268-3.14, p=0.003) and 1.961 (CI 1.183-3.251, p=0.009) respectively. No other disease was found to be significantly associated with male UI in this study (Table 3). 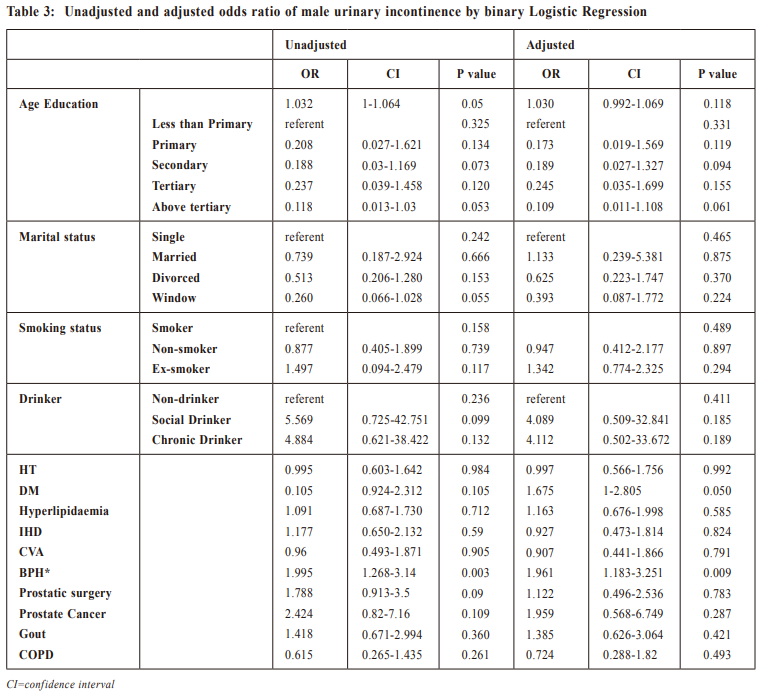 There was a positive correlation between the ICIQ- UI SF score and the KHQ scores, indicating that the quality of life was more severely affected with a higher score in ICIQ-UI SF. There was a strong correlation between the ICIQ- UI SF score with the KHQ domains on incontinence impact (rs=0.707, p < 0.01), severity measures(rs=0.596, p< 0.01), a medium correlation on role limitations (rs=0.395, p < 0.01), physical limitations (rs=0.495, p < 0.01), emotions (rs=0.416, p < 0.01), and a small correlation on social limitations (rs=0.284, p=0.004), personal relationships (rs=0.255, p=0.032), sleep and energy (rs=0.258, p=0.009). The impact on general health perceptions was statistically insignificant (p=0.919) (Table 4). 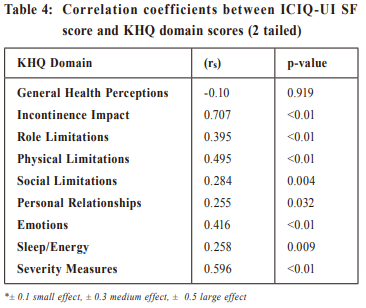
Discussion
|
|

 Standard normal variate, at 5% type 1 error
(P< 0.05) =1.96
Standard normal variate, at 5% type 1 error
(P< 0.05) =1.96