
|
June 2021,Volume 43, No.2
|
Update Article
|
Management of anaemia in primary careShek-ying Lin 連錫營 HK Pract 2021;43:51-57 SummaryAnaemia is a very common problem in primary care and also a serious global public health issue that affects young children and pregnant women. In 2008, WHO estimated that 42% of children under 5 years old and 40% of pregnant women were anaemic and the issue was more severe in the developing world.1 While anaemia of chronic disease is more common in elderly with multiple co-morbidities, iron deficiency in this age group can indicate possible gastrointestinal or gynaecological malignancy. Anaemia is only a presenting symptom with a wide range of underlying causes or conditions, from the common uterine fibroid (UF) to the rare pure red cell aplasia (PRCA) secondary to parvovirus infection. A practical yet comprehensive approach is very important to avoid unnecessary investigation but not missing sinister or readily treatable diagnoses. In this article, the common causes and initial approach to anaemia are reviewed. First line investigations, their interpretation and subsequent work-up in primary care settings are discussed. Special attention is given to iron deficiency anaemia and anaemia of chronic disease and tests to differentiate these two commonest causes, or conditions, presenting with anaemia, updated. 摘要貧血是基層醫療中非常常見的問題,也是影響幼兒 和孕婦的嚴重的全球性公共衛生問題之一。世衛組織估 計,4 2 %的5歲以下兒童和4 0 %的孕婦患有貧血,這一問 題在發展中國家更為嚴重。1雖然慢性病貧血在患有多種 疾病的老年人中較為常見,但這一年齡段的人缺鐵或許 預示著罹患胃腸道或婦科惡性腫瘤的可能。貧血只是一 種症狀表現,其潛在的病因很廣泛,從常見的子宮肌瘤 到罕見的繼發於細小病毒感染的單純紅細胞再生障礙性 貧血均包括在內。採用實用而全面的方法非常重要的, 可以避免不必要的調查,同時又不會漏診兇險或容易治 療的疾病。本文回顧了貧血的常見原因和初步治療方 法,討論了基層醫療機構的一線檢查、檢查結果解讀和 後續工作,尤其關注了缺鐵性貧血和慢性病性貧血,並 介紹了鑒別這兩種最常見原因的最新檢測方法。 IntroductionAnaemia is a condition in which the number of red blood cells or the haemoglobin concentration is lower than normal. The normal haemoglobin concentration varies with age, diet, altitude of residence, smoking, sex, pregnancy and menstruation. The most common causes of, or conditions presenting with anaemia include nutritional deficiencies, particularly iron deficiency anaemia (IDA) and anaemia of chronic disease (ACD) and IDA/ACD frequently coexisted.2 According to World Health Organisation (WHO) criteria, anaemia is defined as a haemoglobin of <13g/dL in men and 12g/dL in women3 though local variations in haemoglobin distribution should be considered. Normal range of haemoglobin used in our Hospital Authority is 11.5-15.4g/dL for women and 13.5-17.3g/dL for men. In Southern Chinese where thalassaemia is common, we usually take a lower limit of normal at 11.5g/dL for women according to our local reference range. Classification of anaemiasAnaemia is commonly classified into three main categories according to the mean corpuscular volume (MCV), namely: macrocytic, normocytic and microcytic anaemia. Table 1 shows a list of the common causes of anaemia, or conditions, according to their MCV.  The in-out approach for classification of anaemia considers red cells as a product and the quantity of haemoglobin will then be a function of the raw materials (nutrition supply), production plant (the bone marrow) and consumption (destruction). Different causes are listed in Table 2. 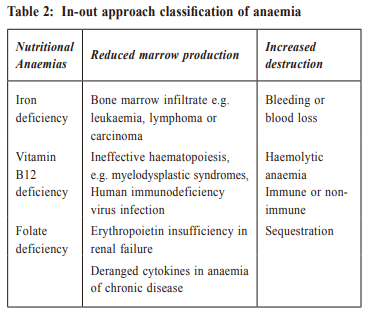 An approach to anaemiaThe diagnostic approach to anaemia in primary care should start with history and physical examination. Afterwards there should be some baseline tests followed by more specific investigations as indicated. A stepwise approach is discussed below. Taking a historyThe severity of symptoms varies with the degree of anaemia and most patients are asymptomatic unless the haemoglobin falls below 10g/dL. Not infrequently mild anaemia is detected during a health check, or a blood test taken for other complaints. Symptoms of anaemia include tiredness, fatigue, malaise, dyspnea on exertion and decreased exercise tolerance. The severity of symptoms depends on the rate of haemoglobin drop; and patients with chronic kidney diseases commonly tolerate anaemia despite a very low haemoglobin. While anaemia from acute blood loss or haemolysis are likely to have more severe symptoms. Symptoms of angina or heart failure may indicate decompensation and need urgent attention. Dietary cause of iron deficiency is more frequent in children, elderly and pregnancy. Folate deficiency is more common in alcoholics and vitamin B12 deficiency in vegetarian. Drug history of anti-convulsants, cholestyramine, sulphasalazine or methotrexate is an infrequent cause of folate deficiency. Chronic kidney disease or other chronic inflammatory diseases are top causes of anaemia of chronic illness. Past history of gastrectomy or intestinal resection should alert the possibility of B12 deficiency. Physical examinationPhysical signs may not be very obvious especially if the patient presented early. Pallor, the diagnostic sign for anaemia may be difficult to detect if haemoglobin is more than 9g/dL. One study investigated the accuracy of pallor at four different sites, namely tongue, conjunctiva, palm and nail bed. The findings suggested that at the haemoglobin cut-off point of 7g/dL, absence of conjunctival pallor and tongue pallor completely ruled out the probability of severe anaemia. However, at haemoglobin cut-off points of 9g/dL, no particular physical site resulted in sensitivity or specificity good enough to rule in or rule out anaemia.4 Most patients will become symptomatic when haemoglobin falls below 7g/dL and urgent referral is warranted. Jaundice may suggest haemolytic anaemia or megaloblastic anaemia which has shortened red cell survival or intramedullary haemolysis. Lymphadenopathy will point to lymphoproliferative disease or other malignancy. Ankle edema is a feature of heart failure and severe anaemia which suggest decompensation. Premature greying of hair often accompanies megaloblastic anaemia and is associated with other autoimmune diseases. Bleeding manifestations such as petechiae, purpura, ecchymosis raise the possibility of thrombocytopenia or marrow failure. Classical signs of koilonychia in iron deficiency or raw beef like glossitis in megaloblastic anaemia are now rarely seen. Standard system examination is required to detect evidence of chronic illness and especially signs of occult malignancy. Hepatosplenomegaly suggests myeloproliferative, lymphoproliferative disease or haematological malignancies. Ataxia, peripheral neuropathy, loss of vibration sense and proprioception may be the presenting features of pernicious anaemia. First-line investigationsA complete blood count (CBC), reticulocyte count with differentials and blood smear is standard. Liver, renal function, lactate dehydrogenase, iron, total iron binding capacity, and ferritin are commonly requested first line work up for anaemia. If chronic inflammatory disease or infection is suspected, C-reactive protein can be considered. The CBC confirms the clinical suspicion of anaemia and the red cell indices direct further investigation. Local laboratory reference ranges that are age and sex specific should be used. The reference ranges for haemoglobin are affected by ethnicity, altitude, nutritional factors and local prevalence of diseases that can cause anaemia. Reticulocyte count gives an indication of the bone marrow erythropoiesis activity, especially its capacity to increase red cell production in response to anaemia. A reticulocyte production index (RPI) is a more accurate reflection of marrow activity than an isolated reticulocyte count5 , because it corrects for the degree of anaemia. A low absolute reticulocyte count in an anaemic patient suggests marrow pathology or anaemia of chronic illnesses. Differential diagnoses are further classified by red cell indices (Table 1) and hints for underlying causes are frequently seen in peripheral blood smear (Table 3). Blood smears morphology of white cells is often the first clue to the diagnosis of haematological malignancy, however a well-trained technologist in haematology is essential for the blood film interpretation.  Subsequent investigations(1) Blood testsFor confirmed iron deficiency anaemia, underlying chronic blood loss from gastrointestinal tract or gynaecological origin must be vigorously sought which often includes upper and lower endoscopy plus gynaecology assessment. Isolated thalassaemia trait seldom has a haemoglobin below 10g/dL and the MCV is usually between 65-70 fL. Common alpha or beta thalassaemia traits are usually identified by a haemoglobin pattern while rarer haemoglobinopathies may need molecular tests for the genetic defect. Lead poisoning is rare unless there is occupational exposure or environmental contamination. Normocytic anaemia needs detailed system review to look for underlying chronic illness, especially malignancy. Mixed anaemia should always be considered if there is a dimorphic blood picture with the concomitant occurrence of microcytosis and macrocytosis despite a normal MCV. In megaloblastic anaemia, we should also check for antibodies against intrinsic factor and parietal cell while upper endoscopy should be considered for atrophic gastritis. Macrocytic anaemia is rarely seen in hypothyroidism though thyroid function test is usually part of the work up of macrocytosis. Rouleaux formation in myeloma can occasionally be misinterpreted as macrocytes by automated cell counters. A high percentage of reticulocytes in haemolytic anaemia will increase the MCV. (2) Bone marrow biopsyBone Marrow (BM) examination is indicated when first line investigations suggest an underproduction e.g. a very low reticulocyte count or abnormal cells detected in blood film. Sometimes when nutritional causes for anaemia are excluded and no chronic disease can be identified or the degree of anaemia is not proportional to the degree of chronic disease, then a marrow biopsy is required to exclude myelodysplasia, hypoplasia or infiltration. Bone marrow aspirate allows morphological assessment, cytochemistry and immuno-staining of blood cells. Trephine biopsy permits better delineation of cellularity and architecture of marrow. Pathology such as granuloma, tumour infiltration and fibrosis is more readily appreciated in trephine biopsy than marrow aspirate. More specialized tests e.g. cytogenetic, immunophenotyping or molecular test are required in individuals suspected of having haematological malignancy6 , therefore specialist opinion should be sought before proceeding to marrow biopsy Common types of anaemia(1) Iron deficiency anaemia (IDA)The total body iron store is around 3-4g in adults. Most of the iron exists as haem in the haemoglobin. One gram is stored in the liver, and a small amount is in the muscle as myoglobin.7 About 20mg – 25mg of iron is needed daily for production of red cells and cellular metabolism and most of the iron in haem is recycled to meet the demand. Men and non-menstruating women lose about 1mg of body iron per day and menstruating women lose an extra 1mg daily on average. Physiological requirements increased rapidly during growth spurt, menstruation, and pregnancy, and therefore iron deficiency is more common in children and pregnancies. Iron absorption from duodenum is upregulated by iron deficiency and downregulated by infection or inflammation. Dietary iron exists in two forms: haem iron and non-haem iron. Fe2+ (ferrous iron) is more readily absorbed than Fe3+ (ferric form). Animal food sources, such as meat, poultry, and seafood contain iron in the haem form, therefore is more readily absorbed than its vegetarian counterpart.8 Serum iron measures the amount of iron bound to transferrin in the plasma. Only a small amount of iron is transferrin bound and there is a large fluctuation of serum iron with dietary intake. The day to day variations are so large that the serum iron results can be misleading and must be interpreted together with the iron binding capacity and ferritin. The total iron-binding capacity (TIBC) determines the amount of iron that can be bound to unsaturated transferrin, i.e. the total number of transferrin binding sites per unit volume of plasma. Unlike serum iron, TIBC or total transferrin sites available do not change rapidly with diet. TIBC will increase in response to anaemia, however, its values do not change until iron stores are depleted. TIBC and transferrin rise in iron loss and fall in chronic disease. Transferrin saturation is calculated by dividing serum iron by TIBC. It is the percentage of transferrin bound to iron. In iron deficiency, the amount of iron is reduced and the TIBC will increase and therefore the transferrin saturation will be reduced. A transferrin saturation of < 15% together with an elevated TIBC is indicative of iron deficiency anaemia. In anaemia of chronic disease, both serum iron and TIBC will decrease but the fluctuation of serum iron can be so large that the 15% cutoff may become misleading. Ferritin is the main iron storage protein in the body, the majority of ferritin is intracellular and the soluble form can be measured in the plasma. Ferritin concentrations vary by age and gender because of menstruation loss. A ferritin concentration of < 15 ng/ml in adults is diagnostic of iron deficiency.9 However, ferritin is an acute phase protein, so it may increase in infection and inflammation. Therefore, a normal ferritin concentration alone does not necessarily exclude iron deficiency. A higher ferritin level of 100 ng/ml is commonly accepted to indicate adequate iron. (2) Anaemia of chronic disease (ACD)Anaemia of chronic disease is a diagnosis of exclusion e.g. in rheumatoid arthritis, anaemia can be caused by iron deficiency after non-steroidal antiinflammatory drug, myelodysplasia due to methotrexate or tuberculosis secondary to the use of biologics. And the list of ACD is ever increasing. Some of the common ones are listed in Table 4.  The pathogenesis of ACD involves ineffective utilization of body iron, reduction in erythropoiesis, and diminished response to erythropoietin stimulation. Though not completely understood, the pathogenesis is thought to be mediated through the actions of tumour necrosis factor, interleukins (IL)-1 and -6 and hepcidin.10 These cytokines and hepcidin, are believed to inhibit iron release from the marrow macrophages to the erythroid precursor cells. The management of ACD is to investigate for the underlying chronic disease and treat accordingly. However, ACD often has overlapping iron profiles with IDA and sometimes both conditions exist concurrently. It is important to identify iron deficiency in this scenario as gastrointestinal or gynaecological malignancy may be missed without searching for the underlying cause for iron deficiency.11 Differentiate iron deficiency anaemia (IDA) and anaemia of chronic disease (ACD)Soluble transferrin receptor indexThe transferrin receptor is a transmembrane cellular protein expressed in cells that utilize iron, and the soluble form is a fragment of the transferrin receptor whose serum level rises in case of iron deficiency. Soluble transferrin receptor (sTfR) has been shown to be an accurate indicator of iron deficiency and is unaffected by concomitant chronic disease and inflammation. Patients with IDA or combined ACD/IDA have significantly higher sTfR and sTfR Index values than subjects with pure ACD. sTfR index is defined as sTfR level divided by logarithm of ferritin concentration. sTfR values > 1. 55 mg / Land sTfR Index values >1.03mg/L were predictive of iron deficiency anemia in the presence of inflammation or chronic disease.12 The combination of ferritin, sTfR and the sTfR Index increases sensitivity to 92%. However, sTfR assay is not available widely. Reticulocyte haemoglobinReticulocytes are the youngest and the freshest red cells released from the bone marrow into the blood and they circulate for 1-2 days then become mature RBC. The reticulocytes haemoglobin content reflects the amount of iron available for haemoglobin production in the bone marrow. Some automated cell counters can generate this value from the cell volume and haemoglobin concentration of the reticulocytes. A cut-off value of reticulocyte haemoglobin was determined as 29.3 pg for female patients with IDA anemia (90.6% sensitivity, 66.7% specificity).13 Haemolytic anaemia (HA)For haemolytic anaemia, the typical laboratory findings include: increased reticulocyte count, unconjugated bilirubin, lactate dehydrogenase and reduced haptoglobin. Blood film may show polychromasia, agglutination and spherocytes. However, not all abnormal laboratory parameters are present, especially in mild and compensated haemolysis. Urine dipstick can be positive for haemoglobin but urine microscopy is negative for red cells if there is intravascular haemolysis. Urine haemosiderin can be detected in chronic intravascular haemolysis such as paroxysmal nocturnal haemoglobinuria.  A positive direct antiglobulin test (DAT) indicates the presence of immunoglobulin IgG or complement (usually C3d) bound to the red cell membrane. Together with the presence of haemolysis, a positive DAT suggests an immune etiology but clinical assessment is required before a diagnosis of AIHA is made because false positive DAT can happen in healthy subjects, hospitalised patients or after blood transfusion.14 The further differentiation of different types of immune haemolysis is beyond the scope of this article. 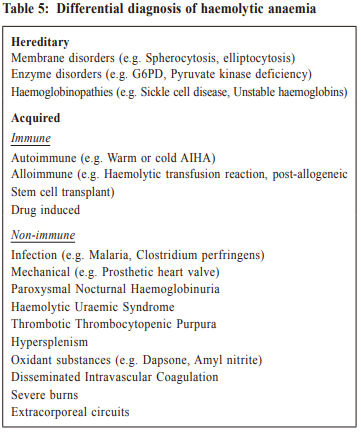 Mixed anaemiaBoth iron deficiency anaemia and thalassaemia are common in Hong Kong and have a low MCV. Megaloblastic anaemia (MA) can be masked by concomitant microcytic anaemia. Delayed diagnosis of vitamin B12 deficiency can result in permanent neurological deficits or memory loss. Therefore, mixed types of anaemia should always be considered. According to a local study, among 272 adult Chinese patients diagnosed to have megaloblastic anaemia caused by vitamin B12 deficiency, 20 or 7.35% of patients (14 definite pernicious anaemia, four probables, two postgastrectomy) had normal or low MCV.15 In the study, all 20 patients had a low reticulocyte index and a widened red cell distribution width (RDW) indicated a maturation disorder. Serum bilirubin and lactate dehydrogenase level reflect red cell turnover rate and are elevated in ineffective erythropoiesis such as in megaloblastic anaemia and thalassaemia. Another telltale sign is the dimorphic blood film which showed the simultaneous occurrence of microcytic and macrocytic cells in the same patient. Treatment of IDAReplacement of ironA daily dose of 100mg to 200mg elemental iron is recommended (e.g. 300mg bd of ferrous sulphate). Different preparation of iron supplement has similar efficacy and metallic taste and constipation are common side effects which often limit its usage. Intravenous iron such as ferric carboxymaltose or iron isomaltoside are indicated in patients with poor tolerance or compliance to oral replacement or there is an urgent need to raise the haemoglobin level e.g. before surgery or acute blood loss.16 Anaphylaxis to intravenous iron is infrequent but it should be given in day care centers where resuscitation facilities are available. Patients with active infection, severe asthma, multiple drug allergies or hyperparathyroidism should avoid intravenous iron and specialist advice is required before iron infusion in patients with rheumatoid arthritis or systemic lupus erythematosus. Response to iron should be evident in 4 weeks. Search for underlying cause of iron deficiency should not be delayed. ConclusionAnaemia is a diagnostic problem that is commonly presented to the general practitioner. There are numerous and varied differential diagnoses of anaemia. Given the diversity of causes, a thorough history, physical examination and systematic laboratory investigation are the key elements towards making a definitive diagnosis. The management should start with a set of baseline investigations to narrow down the list and followed by selected subsequent investigations directed to the subtypes of anaemias. A systematic approach is required to avoid over investigation while not missing treatable causes especially malignancies. Iron deficiency anaemia and anaemia of chronic disease remain the most common causes of anaemia and further study is required to differentiate them.
Shek-ying Lin, FHKAM (Medicine)
Correspondence to: Dr Shek-ying Lin, Haematology Division, Department of
Medicine, United Christian Hospital, 130 Hip Wo Street, Kwun
Tong, Kowloon, Hong Kong SAR.
References:
|
|