
|
March 2021,Volume 43, No.1
|
Original Article
|
A comparison of retention rates of two innovative recruitment methods in smoking cessation interventionKin-sang Ho 何健生,Patrick W Y Fok 霍偉賢,Helen C H Chan 陳靜嫻,Siu-lun Kwok 郭兆倫,Marco C O Lau 劉志安 HK Pract 2021;43:4-8 Summary
Objective:
To compare the effectiveness and retention
rate of two innovative recruitment methods in smoking
cessation intervention
Keywords: innovative recruitment, retention rate, first appointment 摘要
目 標 :
比較兩種新用招募參與戒煙計劃方法的保留率
主要詞彙 : 新用招募方式,保留率,初次約診時間 IntroductionThe smoking of tobacco is the most preventable cause of many illness and premature deaths in the world.1,2 In Hong Kong, each year over 5,000 deaths are attributable to active smoking.3 Quitting smoking is the most effective preventive means to reduce the health burden of many non-communicable diseases. In 2009, the Tung Wah Group of Hospitials Integrated Centre on Smoking Cessation (TWGHs ICSC) has established 8 smoking cessation clinics in Hong Kong under the subvention of the Department of Health, HKSAR. The Centre provides free counselling and pharmacotherapy for smokers who seek help with smoking cessation. In recent years, the service demand for smokers to quit smoking has decreased, and we have to think of new and innovative recruitment methods to attract more smokers to enrol in our services. Cochrane review has already indicated that recruitment methods should be more proactive in nature with more intensive recruitment elements (i.e., those strategies that require increased contact with potential participants).4 In fact, some overseas studies commented that many smokers are ambivalent to smoking cessation in spite of the fact that there are smoking cessation services available, and some of them may default their first appointment. We have to study this phenomenon in order to boost up our recruitment and cessation rate.5,6,7 The main objective of the present study is to evaluate the recruitment effectiveness and retention rate of two innovative recruitment methods. MethodologySince 2017, an active recruitment for smokers was initiated. A mobile truck decorated with big banners went to various busy districts and smoking hotspots in Hong Kong. A nurse and a counsellor stationed in the truck would receive smokers who were interested in smoking cessation. Brief counselling would be given, and methods of smoking cessation were introduced. A one week free supply of nicotine replacement therapy (NRT) was given to those suitable smokers who wished it. At the same time, an appointment would be arranged to attend a formal treatment programme in one of our clinics. The appointment time was given according to the clients’ preference and availability of appointment time slots. A few days were deliberately allowed to lapse so as to allow the clients time to try out the NRT. The concept of NRT sampling was based on a study by Carpenter et al8 who claimed that by providing smokers with free NRT samples, this would encourage them to engage in temporary abstinence, resulting in meaningful change in motivation and self-efficacy, which in turn influence smoking outcomes. We defined engagement as the time the clients volunteered to come up to our truck to give their personal particulars and enrolment into our smoking cessation programme. We coined this as the ‘mobile truck group’. Another recruitment method is the utilisation of QR code. Stickers printed with promotional slogan and a QR code were sent to general practitioners, dentists, hospitals and management offices of public housing estates. They were also stuck onto garbage bins of smoking hotspots on the street. Interested smokers can scan the QR code with their mobile phone and this will direct them to a google form to apply for smoking cessation service. This group was labelled the QR code group. The smokers have to fill in their name, mobile phone numbers, Fagerstrom questionnaire (a measurement of the severity of smoking addiction), the preferred clinic to receive service, the preferred date and time of the first appointment. Their Hong Kong identity card number was not required. We pledged to return calls within two working days to confirm the date of appointment. The appointment time was given according to the client’s preference and available appointment time slot. Recruitments from both groups will receive the same intervention service (i.e. pharmacology plus counselling) for 8 weeks. We collected data from 1 April 2019 to 31 December 2019. Those who came up to our clinics to enrol for service was counted as a successful recruitment. On the day of their first appointment, we captured their basic demographics such as age, gender, education level, marital status, employment status, daily cigarette consumption, previous quit attempt, Fagerstrom score, confidence of quitting and the importance of quitting score. We captured the date of application of service, and also the number of smokers who turned up for their first appointment in both groups. The retention rate is defined as those who had turned up for their first appointment after receiving the NRT sample or after submitting the google form. All smokers who engaged in both recruitment programmes were included in the study, and those who were mentally unstable were excluded. The outcome measures were retention rate and the self-reported abstinence rate at 8th and 26th week. The abstinence rate was defined as 7-day point prevalence of abstinence. Those who were lost to follow- up or could not be contacted would be considered as non-quitters based on the intention to treat principle. Statistical analysisThe demographics and smoking behaviour of the two different groups were compared using the t-test and Chi square test. The Chi square test was used to study the differences between the recruitment and retention rate in both groups. ResultDuring the study period, there were 196 cases who applied (engaged) for service through QR code and 172 cases (88%) who actually enrolled as service users. 427 cases engaged in the mobile truck service and 241 cases (56.44%) actually enrolled in the mobile truck group. Table 1 shows the demographics and smoking behaviour between the QR code group and the mobile truck group. As compared with the mobile truck group, the QR Code group had more female and less male; more subjects had post-secondary school education level and in the 21-40 age group; higher Fagerstrom score; more previous quit attempts; higher rating on importance of quitting and these were all noted to be of statistical significance. The quit rate of the QR code group at 8th week was 57.56% and 26th week 50%; the quit rate of the mobile truck group at 8th week was 48.54% and 26th week 41.9%. Statistically, there was no difference in quit rates between the two groups. 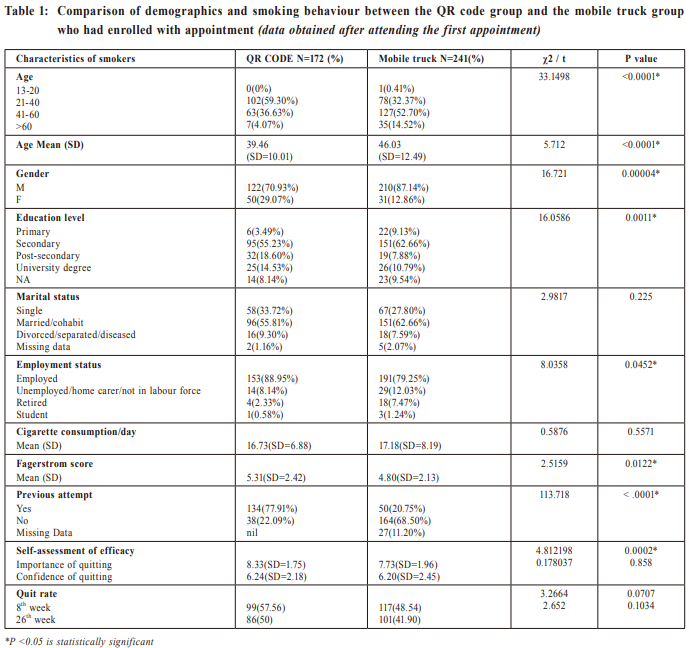 Table 2 shows the relationship of time elapsed between application/engagement date and the first appointment date for both groups and the attendance rate. It demonstrated that the QR code group had a shorter time lapsed between application/engagement date versus first appointment date as compared with the mobile truck group. Its retention rate was higher and was noted to be of statistical significance. If the time lapsed between the application date and the first appointment was one week or less, the retention rate was significantly higher statistically in the QR group. In the QR code group, 111 (56.64%) subjects made the application during our office hours, whereas 85 (43.36%) made the application during non-office hours as seen in Table 3. As can be seen, those who made their bookings within non-office hours, about 59% of application were made in the latter half of the day (i.e. 9 pm till 6 am of the next morning). 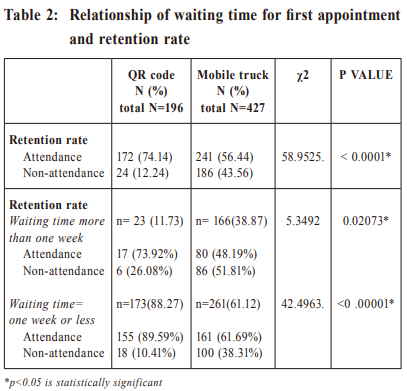 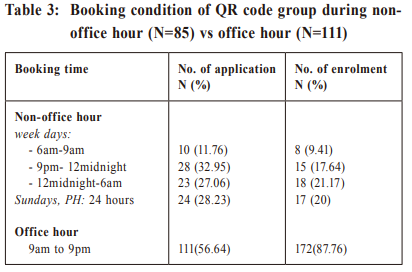 DiscussionIn the current study, we compared the recruitment effectiveness and retention rate of two innovative recruitment methods. Recruitment with NRT sampling was noted to be effective via previous overseas studies.9 A local study on out-reaching programme with NRT sampling has also proven to be effective.10 However, there is apparently no report on any study using QR codes as a recruitment method. QR code recruitment is a semi-active recruitment method. It is convenient to make contact with us without direct dialog. It is user-friendly for those who do not like person-to-person calls and for the younger generation who prefer to use their mobile phones to connect with others. It can be seen from our study that many users were in the age group of 21-40 (55.7%). This method uses less manpower and is more cost effective since the clients are responsible for filling out a google form on their smoking habits and personal particulars. The demographic and smoking habit of both groups were somewhat similar in terms of marital status, cigarettes consumption per day, confidence score on quitting, with significant differences in gender and employment status. The retention rate is significantly related to the time lapsed for the first appointment. Time lapsed of one week or less can definitely lead to more retention. This finding is important once smokers express their intention to quit. It is preferable to give an early appointment as far as possible so as not to allow their zeal for quitting to die down. Smokers’ motivation to quit can change quickly, depending on the stage of change, as described by the “Transtheoretical model”.11Some studies also showed the impact of waiting time on the attendance of the first appointment on treatment programmes other than smoking cessation.12,13,14 Another advantage of the QR code recruitment is that it can be conducted 24 hours a day and during public holidays at the clients’ convenience, as shown in Table 3. All we have to do is to collect the google form and give an appointment at our own pace. This can be seen from our data on google form submission that many cases submitted their request after office hours and on Sundays. Smokers or clients have different routines. Some may work long hours far beyond normal 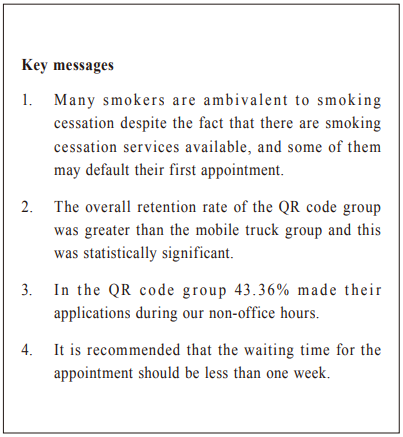 office hours, which may lead to the deprivation of service if the QR code recruitment service was not in place. Certain types of smokers needs to be “won over” as “potential clients” for an intervention programming aiming at addressing their specific needs. This study serves to demonstrate that the QR code recruitment and mobile truck with NRT sampling were effective methods to recruit smokers with quit rates of 50% and 41.9% at 26th week respectively. The major limitation of this study was that it was not a randomised control trial and hence there was no control group for comparison. The comparison groups were different in terms of characteristics of the smoking subjects and the method of recruitment, e.g. with or without NRT. The mobile truck recruited smokers from various busy districts of the Territories and also smoking hot-spots, hence some ambivalent smokers might be recruited via this method. QR code users were attracted via advertisements and publicity campaigns and therefore this method may attract different smokers with more motivation to quit smoking. We are trying to compare these two methods via real life situations, and hence cannot controlled all possible confounding factors. The abstinence rate is self-reported and there is no biological validation. Another important limitation is that for the mobile truck group several-days of time lapse (though only less than one week) is deliberated to allow the client to try out the NRT whereas no timelapse was deployed for the QR code group. In this study, other possible factors leading to non-attendance have not been evaluated.
Conclusion
|
|