
|
March 2021,Volume 43, No.1
|
Update Article
|
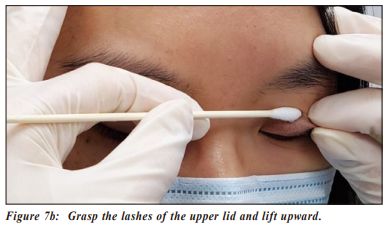
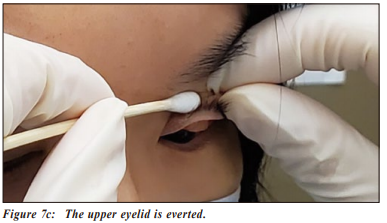
Approach to red eye and other acute conditions in primary careShiu-ting Mak 麥兆婷 HK Pract 2021;43:13-20 SummaryAcute eye redness may occur at any age group. While some red eyes are asymptomatic and may even resolve without treatment, some may be severe resulting in permanent visual loss if not treated in time. Primary care physicians are often the first line of contact for patients presenting with red eye(s) or other acute conditions. This article aims to review the management of acute eye conditions causing redness and pain encountered in daily primary care practice. 摘要急性眼紅可在任何年齡組別發生。部分眼紅患者無病徵, 並可自行痊癒,但部分患者如無接受適時治療,可嚴重至 永久視力受損。基層醫生經常是眼紅或其他急性疾病患者 最早接觸的醫護人士。本文回顧在日常基層醫療中急性眼 紅疾病的診療。 IntroductionAcute red eye is com monly due to infection, inflammation, trauma, subconjunctival haemorrhage and acute glaucoma. Redness can affect one or both eyes, and may occur at any age. Depending on the cause, management and prognosis vary in different cases. This article reviews the management of acute red eye commonly encountered in primary care practice. Infections of eyelidsHordeolum and ChalazionHordeolum is a red painful swelling of the eyelid margin that is usually caused by a bacterial infection (Figure 1). 1 It commonly occurs following blockage of oil glands with secondary bacterial infection, most often Staphylococcus aureus. External hordeolum or stye is the acute infection of the Gland of Zeis and the lash follicle. Internal hordeolum is the infection of the meibomian gland.1 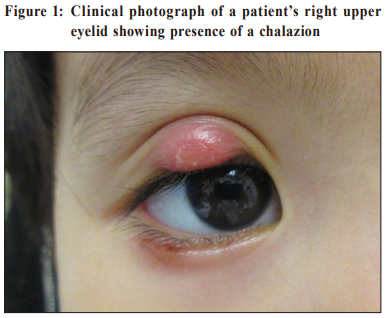 The infection may spread to neighbouring ocular tissues and result in preseptal cellulitis. Persistent stye may lead to chronic inf lammation resulting in formation of a chalazion. Initial treatment is mainly conservative, involving application of warm compresses several times a day. Better eyelid hygiene is beneficial. A topical antibiotic may be prescribed in conjunction to prevent spread of infection; it may reduce healing time by fighting against the causative bacterial infection and reducing inflammation.1 If the condition is severe or resistant to conservative management, systemic antibiotics or surgical incision and drainage may be required. BlepharitisBlepharitis is commonly a result of a Staphylococcal infection. It may also be associated with skin conditions such as seborrhroeic dermatitis. Demodex, a mite that lives in or near hair follicles, may occasionally be a cause of persistent blepharitis. Patients with blepharitis usually present with red eyelids, itchiness and irritation. Sometimes, crusts and scales may be found adhering to the base of the eyelashes (Figure 2).The main stay of treatment of blepharitis involves promotion of eyelid hygiene and keeping the lids free from crusts and scales. Warm compresses and light scrubbing of the eyelids are beneficial. Lid scrubs consisting of saline or diluted mild shampoos can be applied to the affected area. Topical antibiotics provide symptomatic relief and were found to be effective in clearing bacteria from the eyelid margins. In severe cases, oral antibiotics such as doxycycline may be required. Younger children should be prescribed erythromycin instead. 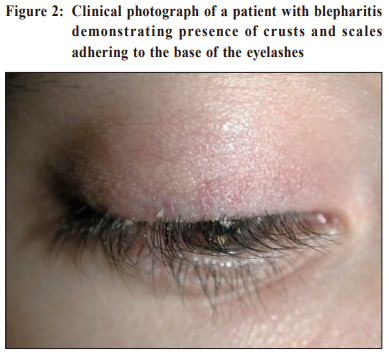 Infections of the Lacrimal SystemDarcyocystitisDacryocystitis is infection of the lacrimal sac. It often occurs in patients with underlying nasolacrimal duct obst r uction. Dacr yocystitis develops when bacterial overgrowth occurs in the stagnant f luid of the lacrimal sac. Staphylococcus and streptococcus are commonly involved. Patients with dacryocystitis present with a painful swelling over the nasal aspect of the lower eyelid (Figure 3). They often have a history of chronic tearing due to underlying nasolacrimal duct obstruction. Purulent discharge may be expressed by applying pressure over the lacrimal sac. It may progress into preseptal cellulitis or even orbital cellulitis, and recurrences are common. Treatment includes topical and systemic antibiotics. Surgical drainage is the definitive treatment. Incision and drainage of the abscess involves expression of pus, irrigation of the lacrimal sac with hibitane solution, and packing of the lacrimal sac. In patients with frequent recurrences, the ultimate treatment would be dacryocystorhinostomy to recanulate the nasolacrimal duct. 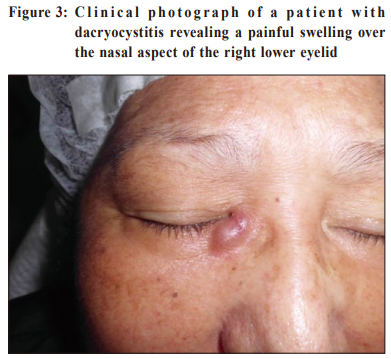 Infections of conjunctivaConjunctivitisConjunctivitis is the inflammation or infection of the conjunctiva and is characterised by dilatation of the conjunctival vessels, resulting in hyperaemia and oedema of the conjunctiva, typically with associated discharge. 2 Conjunctivitis is most commonly viral, bacterial or allergic in nature. Majority of conjunctivitis are initially treated by primary care physicians rather than ophthalmologists. 3 It has been reported that approximately 70% of patients with acute conjunctivitis presents to primary care and emergency care, whereas 20% present to an ophthalmologist or optometrist.4 Differentiation between viral and bacterial conjunctivitis may not be easy. In general, purulent or mucopurulent discharge is often due to bacterial conjunctivitis, whereas a watery discharge is more characteristic of viral conjunctivitis.3 Viruses cause up to 80% of all cases of acute conjunctivitis3 , and is most commonly due to adenovirus.4 Viral conjunctivitis is often bilateral, spreads through direct contact, and is highly contagious especially among children. Never theless, viral conjunctivitis is usually mild and self-limiting. No effective treatment exists, but artificial tears and topical antihistamines may provide symptomatic relief. Patients should be taught to avoid touching their eyes and sharing their towels with others. Frequent handwashing is beneficial. Patients should also be advised of the possible prolonged disease course in terms of weeks. As for bacterial conjunctivitis, the most common pathogens in adults are Staphylococcal species, followed by St re ptococcu s pneu mon iae a nd Haemoph ilu s influenzae. Whereas in children, the disease is often caused by Haemophilus inf luenzae, Streptococcus pneumoniae, and Moraxella catarrhalis.5 Apart from redness, pur ulent or mucopur ulent discharge and chemosis are typical of bacterial conjunctivitis. In hyperacute bacterial conjunctivitis caused by Neisseria gonorrhoeae, patients present with severe copious purulent discharge and decreased vision, often accompanied by eyelid swelling, pain and preauricular adenopathy. Prognosis is worse and progression is rapid, with a high risk of corneal involvement and even perforation. Treatment of bacterial conjunctivitis involves use of topical antibiotics. In cases where gonococcal infection is suspected from history and clinical sig ns and sy mptoms, t reat ment requi res intramuscular or intravenous ceftriazone. It is an ocular emergency and should be managed in a timely manner to prevent the occurrence of complications. The patient should also be screened for possible sexually-transmitted diseases. Chlamydial conjunctivitis is a sexually transmitted disease and occurs most commonly in sexually active young adults. The disease is usually transmitted through hand-to-eye spread of infected genital secretions. Neonatal conjunctivitis caused by Chlamydia trachomatis is characterised by erythema of the eyelids and conjunctiva with pu r ulent eye discharge. It typically occurs between 5 and 14 days of birth. Furthermore, up to 20% of neonates exposed to chlamydial infection during bir th can develop pneumonia, and evidence of conjunctivitis is found in approximately 50% of these cases.6 Patients suffering from allergic conjunctivitis often have concomitant history of asthma, allergic rhinitis and eczema. Hence, history taking is important. In addition to the common symptoms of eye redness, itching and tearing, there will be presence of conjunctival papillae. Treatment involves the use of artificial tears to rinse away allergens, thereby relieving the symptoms. In addition, antihistamine eyedrop provides symptomatic relief, and mast cell stabiliser can be used for prevention as the condition may be recurrent especially in patients with underlying atopy. In severe cases which do not respond to the above treatment, referral to ophthalmologists is recommended as a mild topical steroid may be necessary. Infections of corneaKeratitisKeratitis can be caused by bacterial, viral, fungal, parasitic or amoebic infection. In general, patients with keratitis present with a painful red eye, reduced vision and photophobia. The cornea may show a localised ulcer or abscess, and in severe cases the cornea may be diffusely edematous and hazy. By applying fluorescein stain to the cor nea, the ulcer will appear yellow under normal light and green under cobalt blue light. Conjunctival involvement (i.e. keratoconjunctivitis), is not uncommon. Keratitis is an ophthalmic emergency and deserves immediate treatment and refer to an ophthalmologist. Nevertheless, the cause of keratitis must be identified before commencing treatment. While some therapies are beneficial in certain situation, they may worsen the condition in others. Viral keratitisViral keratitis is commonly caused by her pes simplex virus (HSV). Customarily the virus produces painful, thin, linear, branching lesions on the corneal epithelium with club-shaped terminal bulbs at the end of each branch, known as a dendritic ulcer(Figure 4). 7 Typically, treatment of HSV epithelial keratitis involves use of acyclovir eye ointment. Systemic administration of acyclovir such as in its oral for m has not been shown to be beneficial. Furthermore, use of steroid eyedrops is contraindicated in HSV epithelial keratitis, and i nappropr iate t reat ment can worsen cor neal inflammation and contribute to permanent visual loss.8 Viral keratitis may also be caused by varicella zoster virus (VSV). Herpes zoster ophthalmicus (HZO) is a reactivation of the VSV involving the ophthalmic division of cranial nerve V. Ocular involvement occurs in approximately 50% of HZO patients in the absence of prompt antiviral therapy.9 Treatment requires the use of systemic antiviral drugs. 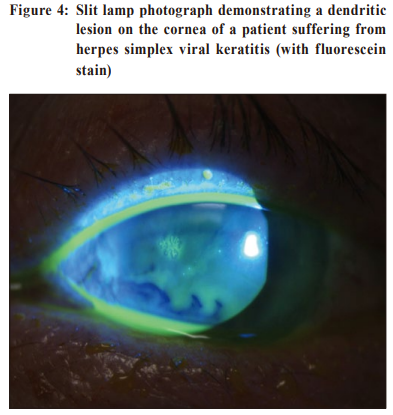 Fungal keratitisFungal keratitis usually occurs in patients with a histor y of trauma particularly due to vegetative matter such as a tree branch. It also affects eyes with chronic ocular surface diseases. In addition to the common symptoms of eye redness, pain, photophobia and tearing, careful examination reveals the presence of a corneal stromal gray-white infiltrate with feathery border, sometimes with satellite lesions. Treatment requires the use of topical antifungal eyedrops but the prognosis is often poor. All cases of suspected fungal keratitis must be referred urgently to ophthalmologists for management. Contact lens keratitisContact lens wear is a known predisposing factor for microbial keratitis. Pseudomonas aeruginosa is the most commonly recovered causative organism in contact lens-related keratitis, followed by Gram-positive bacteria, fungi and acanthamoeba.10 Patients present with eye pain, redness, photophobia, and tearing.Patients often reveal a history of poor contact lens hygiene, overnight contact lens wear, and swimming or taking a hot water bath while wearing contact lenses. Physicians must rule out contact lens related keratitis in every contact lens wearer attending for eye redness. Once contact lens keratitis is diagnosed, patients should refrain from contact lens use immediately. A corneal culture is often taken by ophthalmologists before starting intensive topical antibiotics. Sometimes admission is required for application of intensive fortified antibiotics and close monitoring. Treatment of acanthamoeba is unfortunately often ineffective. In severe non-resolving cases, the cornea may perforate necessitating corneal transplantation. Infection of eyeballEndophthalmitisEndophthalmitis refers to severe int raocular inf lammation and the outcome is often devastating, resulting in marked visual loss and even blindness. It usually occurs as a result of a microbial infection. It can be due to exogenous or endogenous causes. Exogenous endophthalmitis is caused by inoculation of microorganisms from the external environment i nto the eyeball. It most com monly occu rs as a complication of penetrating eye trauma and ocular surgery, including but not limited to cataract surgery.11 The risk of postoperative endophthalmitis following cataract surgery has been progressively decreasing in recent years because of moder n small-incision cataract surgery and widespread use of intraoperative antibiotics. The incidence is now between 0.05% and 0.07%.12 Endogenous endophthalmitis is caused by the haematogenous spread of infectious organisms from distant sites of the body, with Klebsiella urinary tract infection and liver abscess being the most common among the local population.13 Patients with endophthalmitis present with blurring of vision, eye pain, eyelid swelling, conjunctival redness and oedema, and hypopyon, which is inflammatory cells seen as a layer of white-yellowish exudate in the lower part of the anterior chamber of an eye. B-scan ultrasound, a brightness scan commonly used in the ophthalmology field, shows the presence of hyperechogenic opacities in the posterior chamber of t he eyeball i nd icat i ng v it reous a nd poster ior involvement. Endophthalmitis is initially suspected based upon the clinical presentation, and supported by a history of recent operation for exogenous cases, subsequently confirmed with laboratory testing of the vitreous or aqueous humor.14 Treatment of endophthalmitis includes intraocular sampling and intravitreal injection of antibiotics. If no improvement is seen, vitrectomy is performed. Despite treatment, the prognosis of endophthalmitis is poor leaving very limited visual function in most patients. Almost half will result in permanent blindness.13 With disease progression and uncontrolled infection, evisceration is required. Therefore, early diagnosis and treatment is extremely important in preserving useful vision for patients. InflammationUveitisUveitis is inf lammation of one or all parts of the uveal tract, including the iris, the ciliary body, and the choroid. It is often idiopathic, but may also be associated with autoim mu ne diseases such as ankylosing spondylitis, and systemic inf lammatory diseases such as Crohn’s disease. Patients with uveitis present with eye redness, pain, light sensitivity, blurred vision, and may witness dark, floating spots or floaters. To distinguish uveitis from conjunctivitis, notice where the conjunctiva is most red. In uveitis, the conjunctiva is most red at the border of the ir is, whereas in conjunctivitis, the redness involves the entire conjunctiva. Furthermore, careful examination of the uveitic eye may show the presence of posterior synechiae of the iris and keratic precipitates on the cornea (Figure 5). In addition, a history of underlying systemic autoimmune or inf lammatory disease also points towards the likelihood of uveitis. Treatment of uveitis involves the use of steroids, either topically in mild forms or systemically in severe cases.  TraumaCorneal abrasionCorneal abrasion indicates a scratch or break on the surface of the cornea. It is most often a result of trauma to the ocular surface, with the most common cau se bei ng poked by a finger or foreign body. Symptoms of corneal abrasion include eye redness, severe pain, tearing, and photophobia, likely supported by a history of trauma to the eye. The area of the abrasion shows up when fluorescein stain is applied to the eye during examination (Figure 6). It is treated with lubricants to promote epithelial healing. Antibiotic eyedrop is often prescribed to prevent secondary bacterial infection. There has been heated debates on whether to patch an eye with corneal abrasion. It has been proven that treating simple corneal abrasions with a patch does not improve healing rates on the first day post-injury and does not reduce pain.15 The abrasion usually heals with the resolution of symptoms within a few days. Foreign bodyForeign body injury of the eye occurs either at work, at home, or at leisure. Foreign bodies most commonly adhere onto the cornea. However, it may also be trapped in the upper fornix underneath the upper eyelid. Hence, it is always necessary to evert the upper eyelid for a proper examination in patients presenting with foreign body injury of the eye. To evert the upper eyelid, the patient should look down with both eyes open. Depress the mid-portion of upper lid from the side using a cotton tip. Grasp the lashes of the upper lid and lift upward (Figure 7a-c). 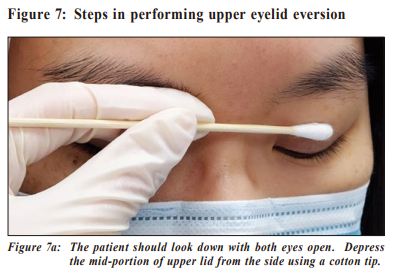
Corneal foreign bodies may cause corneal abrasion resulting in similar sy mptoms. Once identif ied, the foreign body should be removed. The choice of technique will depend on the nature of the foreign body.16 Superficial foreign bodies with no surrounding corneal reaction can often be removed using a cotton tip soaked with local anaesthetic or saline. For more deep seated foreign bodies, needles or drills will be required and removal may better be performed by an ophthalmologist. Irrigation of the ocular surface and the fornices can be performed after the procedure to wash out any residual loose foreign body material. Topical antibiotics eyedrops should be prescribed to prevent secondary bacterial infection. Subconjunctival haemorrhageSubconjunctival haemorrhage occurs when blood vessels break under the conjunctiva. The blood gets trapped as it cannot be quickly absorbed by the conjunctiva. The redness is localised and well demarcated (Figure 8). Despite its redness, it seldom causes other discomfort and is often recognised only when the patient looks into the mirror or is noticed by others.  Subconjunctival haemorrhage can be due to external causes such as trauma to the eye, rubbing of the eye, violent coughing or powerful sneezing, vomiting and straining. However, it can also be related to systemic medical conditions such as hypertension, blood clotting disorders, and use of antiplatelets or anticoagulants. Treatment is not required for subconjunctival haemorrhage, and the blood will gradually resolve over two to three weeks. Nevertheless, it is valuable to check the patient’s blood pressure, and perform blood tests for platelet count and clotting function in recurrent cases. Intra-ocular pressureAcute angle-closureAcute angle-closure (AAC), also known as acute angle-closure glaucoma, is an ocular emergency due to its acute presentation, need for immediate treatment, and well-established anatomic pathology.17 Rapid diagnosis, im mediate inter vention, and timely refer ral have significant effect on the patient’s outcome and morbidity. Apart from eye redness, patients with AAC often present with nausea, vomiting and headache due to a rise in intraocular pressure. They also complain of blurring of vision. There may be a known family history of the same condition. Some patients may reveal the use of “over-the-counter” flu medication purchased by themselves which bear the side effect of pupil dilatation, hence triggering the AAC. Patients with AAC should be treated immediately with systemic diamox and other intraocular pressure lowering eyedrops. Laser or surgical treatment may be required. Diagnostic algorithmHistoryDetailed history taking and careful physical examination may help to identify the cause of redness in patients presenting with a red eye. During history taking, the following questions would help to reach the initial diagnosis:
Physical examinationDuring physical examination, the following associated signs and symptoms should be considered:
When to promptly refer to specialists?Various clues from history taking and several clinical signs and symptoms warrant prompt referral to an ophthalmologist. It is important to bear in mind that reduction in visual acuity may indicate a more serious underlying cause of red eye.
 Some ot her causes of acute red eye such a s dacryocystitis, keratitis, uveitis, foreign body injury etc will also need early referral to an ophthalmologist for management. Conditions such as chalazion, blepharitis, mild conjunctivitis or subconjunctival haemorrhage can be managed by a general practitioner or family physician. Nevertheless, in case of doubt or when conditions are refractory to treatment, these patients should also be referred to ophthalmologists for further assessment. ConclusionFor patients with eye redness, many a time when medical care is sought, a general practitioner or a family physician is consulted before an ophthalmologist. It is therefore important for primary care physicians to be familiar with the common eye conditions causing eye redness encountered in daily practice. While many causes of eye redness such as subconjunctival haemorrhage and blepharitis are relatively mild and may even resolve spontaneously without treatment, some causes may be severe and may result in permanent visual loss if treated inappropriately. Asking key questions and performing a proper eye examination will help to distinguish the cause of the redness, and to determine whether urgent ophthalmologic assessment is necessary. In case of doubt, a timely referral to an ophthalmologist is warranted.
Shiu-ting Mak, MBChB(CUHK), MPH(CUHK), FRCSEd(Ophth), FHKAM(Ophthalmology)
Correspondence to: Dr Shiu-ting Mak, Department of Ophthalmology, United
Christian Hospital, 130 Hip Wo Street, Kwun Tong, Kowloon,
Hong Kong SAR.
References:
|
|