
|
December 2022,Volume 44, No.4
|
Update Article
|
Antibiotic allergy in Hong KongValerie Chiang 姜穎彤, Maegan HY Yeung 楊瀚欣, Philip H Li 李曦 HK Pract 2022;44:98-105
SummaryAccurate assessment and documentation of allergies is paramount to gatekeeping the wellbeing of patients. While failing to label true antibiotic allergies can have deleterious and potentially fatal outcomes, the heaviest burden falls upon those with false beta-lactam (BL) allergy labels living with the lifelong ramifications of inferior broad-spectrum antibiotic treatment unnecessarily. Importantly, mislabelling of antibiotic allergies exacerbates antibiotic resistance and hampers COVID-19 vaccine uptake. Despite the prevalence of mislabelled antibiotic allergies, most patients are not appropriately retested and stratified for risk. The protocol-driven model of the Hong Kong Drug Allergy Delabelling Initiative (HK-DADI) provides a multidisciplinary platform to tackle this issue of delabelling unnecessary drug allergy labels with collaborative efforts from primary care and allied health professionals. With increase in awareness and further multidisciplinary collaboration, reclaiming BL antibiotics to further improve antibiotic stewardship and overall patient health can be well within reach.
摘要準確評估和記錄過敏對於保障病人健康至關重要。 雖然未能標記真正的抗生素過敏可能導致傷害甚至造成 危害生命的後果,但是無 (BL) 過敏的人身上的假過敏標 簽,會成為他們沉重的負擔,導致不必要地使用劣質廣 譜抗生素治療影響終生。重要的是,抗生素過敏的錯誤 標簽會加劇抗生素耐藥性並且阻礙 COVID-19 疫苗的吸 收。盡管錯誤標簽抗生素過敏很普遍,然而大多數患者 沒有做重新測試和風險評估。香港藥物過敏去標簽計劃 (HK-DADI) 提供了一個多學科平臺,通過基層醫療與其 他醫療專職人員的協作努力,解決去除不必要標簽的問 題。伴隨認知的提高和多學科進一步合作,通過回收β內酰胺 (BL) 抗生素改善抗生素管理,整體患者健康可以 迅速提升。IntroductionAntibiotics are frequently associated with a variety of adverse drug reactions and allergies. 1 However, many documented antibiotic allergies are based on vague symptom recollection or misinterpretation of non-immunological adverse events as allergies. Such “allergy” labels are rarely clinically verified or rechallenged.2 The mislabelling of antibiotics allergies, and that of beta-lactam antibiotics (BL) in particular, pose threats to patient wellbeing and global health, especially in light of the COVID-19 pandemic. This article provides an overview of antibiotic allergies, the situation in Hong Kong, and initiatives in place to mitigate the issue of misdiagnosed allergies. What is antibiotic alleregy ?Not all adverse drug resction (ADR) are drug allergies. Unfortunately, the terms “adverse drug reaction”, “drug hypersensitivity” and “drug allergies” are often mistakenly used synonymously. ADR refers to any “appreciably harmful or unpleasant reaction” associated with the use of a medical product regardless of aetiology.3 Drug hypersensitivity reactions (DHR) refers to any immune-mediated response to a drug.4 Drug allergies have traditionally described IgE-mediated reactions, but have recently expanded to include various non-IgE mediated reactions.5 The majority of ADRs (75-80%) are classified as (1) type A: predictable, dose-dependent and non-immunological; (2) type B: unpredictable, dose-independent reactions, or “off-target” reactions, which can be immune-mediated or non-immune mediated. 6-10% of these ADRs are mediated by antibodies or immune cells, and are considered true DHRs.6 DHRs can be categorised in four categories under the Gell and Coombs classification7 , which correlates onset time and clinical manifestations with causative immune mediators: (i) Type I IgE-mediated reactions, (ii) Type II IgM or IgG-mediated cytotoxic reactions and (iii) Type III immune-complex mediated reactions, are all mediated by antibodies. (iv) Type IV hypersensitivity is cell-mediated, and can be further subdivided into “IVa” – “IVd” reactions, based on T-cells involved and cytokines/chemokine mediators. Clinically speaking, DHRs can be divided into “immediate” (<1hr) and “delayed” (>1hr) based on time of reaction onset after last drug administration8, which broadly distinguishes type I IgE-mediated hypersensitivity from type IV and other hypersensitivity reactions respectively (Table 1). In addition to type I and IV hypersensitivity, the rarer type II and type III reactions are also considered true DHRs. 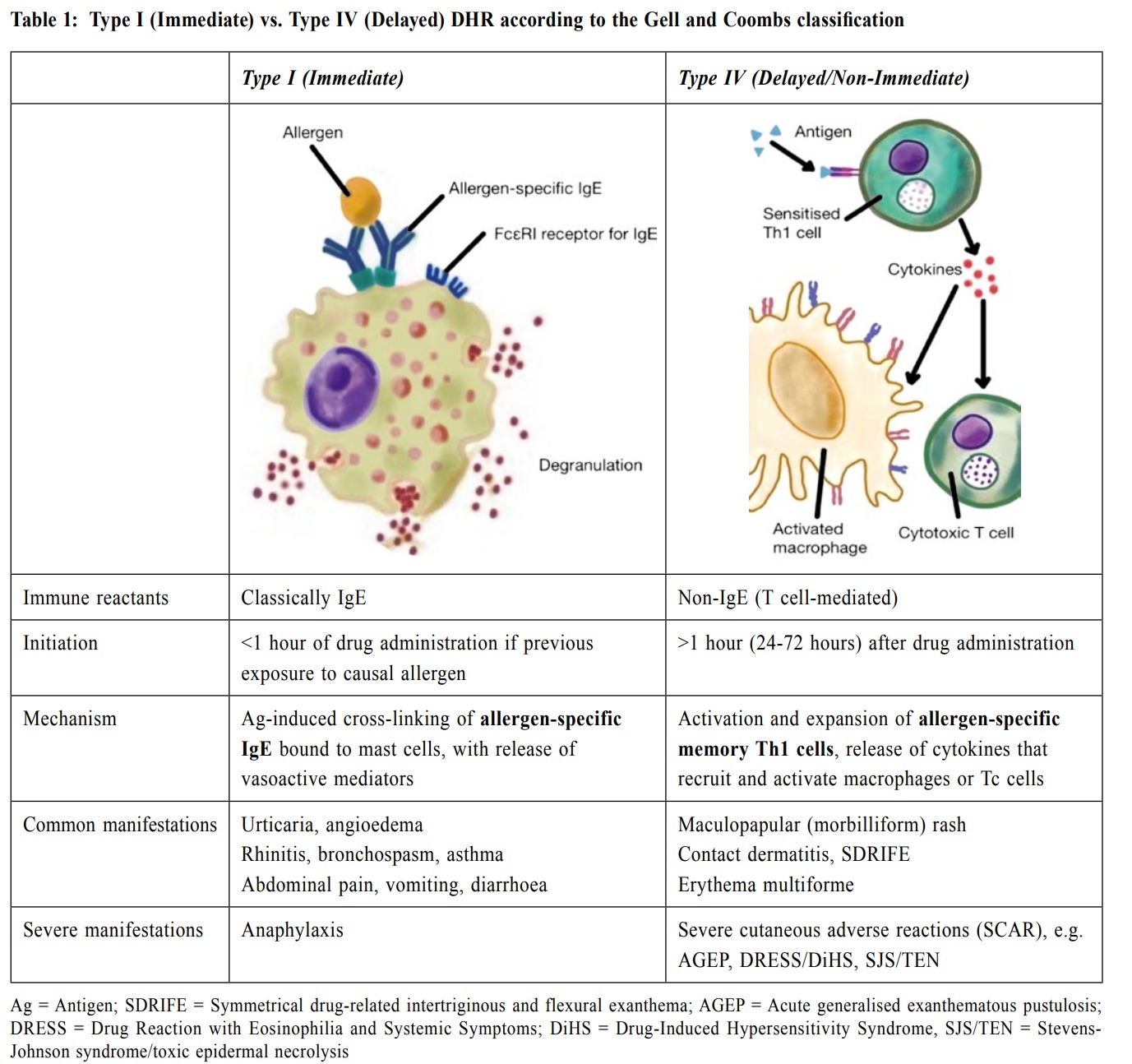
(I) Immediate hypersensitivity reactions Immediate type I hypersensitivity is caused by drug-specific IgE, which are generated from previous exposure to the offending drug and bind to mast cell and basophil FcεRI receptors after formation. Upon re-exposure, the cross-linking of drug-antigen to prebound IgE on the surface receptors activates mast cells, resulting in rapid degranulation and release of vasoactive mediators. Urticarial rash is a hallmark of mast cell degranulation, along with angioedema, pruritus, conjunctivitis, wheezing and gastrointestinal symptoms. In severe cases, anaphylaxis may occur resulting in life-threatening multi-organ damage. Commonly implicated drugs include BL antibiotics, neuromuscular blocking agents, quinolones, and platinum-containing chemotherapy drugs.9 There are two clinically-relevant points to note regarding type I hypersensitivity:
(II) Delayed hypersensitivity reactions The most common mechanism of delayed DHR is type IV hypersensitivity, which is mediated by antigen-specific effector T cells. Type IV hypersensitivity reactions are orchestrated by cytokines released by Th1 CD4 cells in response to antigen. Macrophages recruited to the site of inflammation by chemokines present antigen to T cells and amplify the response. Interferon (IFN)γ and tumour necrosis factor (TNF) α activate macrophages, increasing the release of inflammatory mediators. The timing of reaction onset varies and depends on various factors, including clonicity of T-cell activation13, dose and duration of treatment 14, presence of viral coinfections15 and HLA associations.16 Type IV T-cell reactions primarily present with cutaneous manifestations, as the skin barrier houses a large repository of primed memory-effector T-cells. Most common drug-induced cutaneous reactions are relatively mild. However, severe cutaneous adverse reactions (SCAR - such as SJS, TEN, DRESS and AGEP) can be triggered by superantigen-like stimulation and can be life-threatening due to massive cutaneous necrolysis. At a glance: antibiotic allergy on Hong Kong -ADRs exert a major burden on the healthcare system, complicating 10-20% of hospitalised17 and 23% outpatient cases18 globally. DHRs comprise up to 20% of all ADRs and account for 38%-58.8% of fatal anaphylaxis.19 In Hong Kong, drug allergies are reported in 6% of the general population and 14% of hospitalised patients (Figure 1). 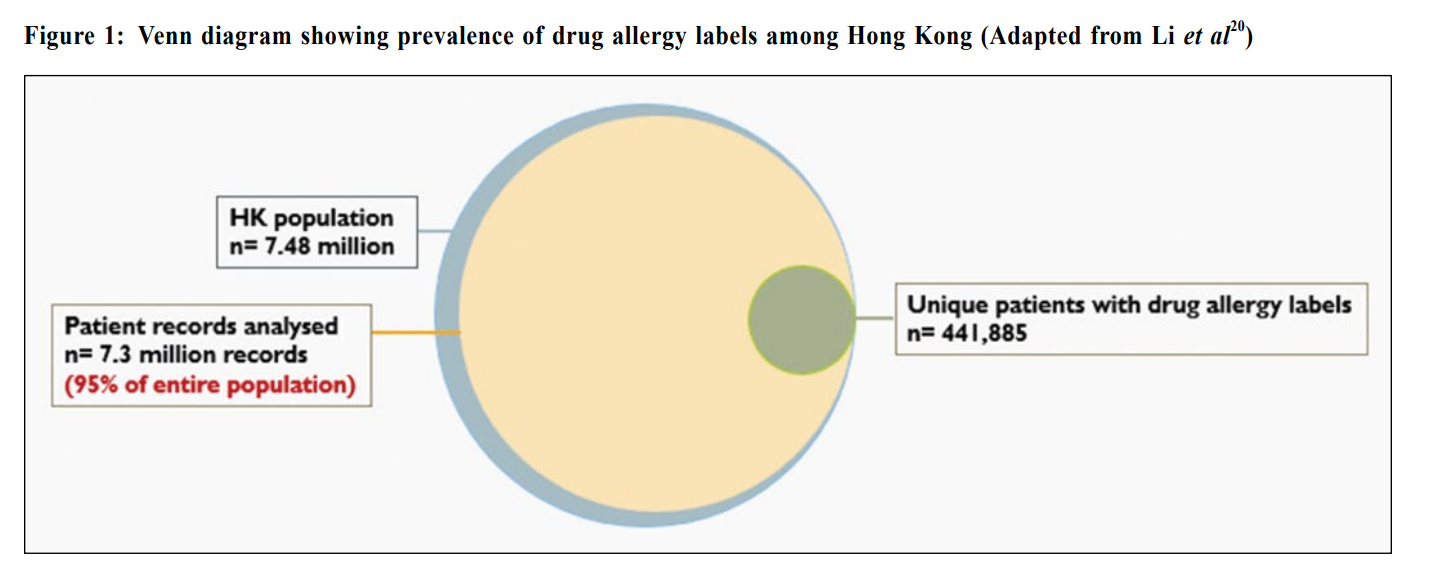
Systemic anti-infectives (32%) are the most common drug allergy labels, followed by central nervous system medications such as analgesics and opioids (22%), eye medications (9%) and cardiovascular/hematopoietic medications (9%). (Figure 2) 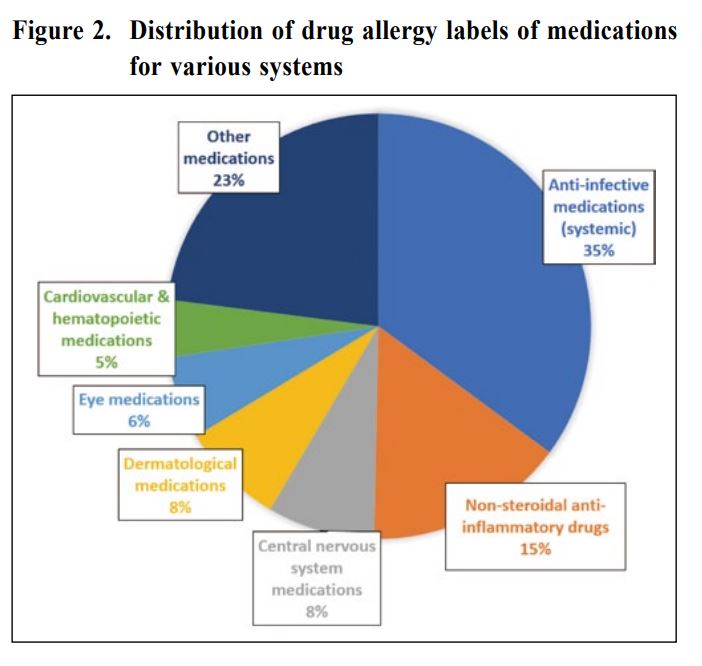
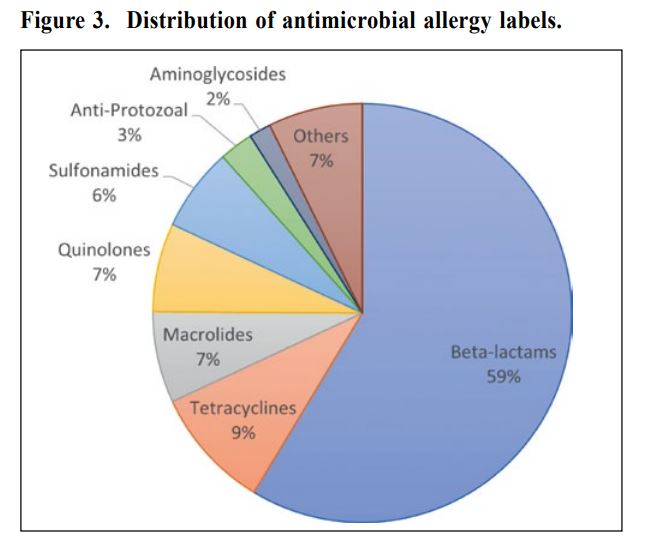
Within antimicrobial drug allergy labels, the
vast majority are attributed to Beta-lactam antibiotics
(59%), followed by tetracyclines (9%), macrolides
(7%), quinolones (7%) and sulphonamides (6%). Beta-lactam antibiotics (Figure 3) are the most widely used
class of antibiotics, and most frequently associated with
drug allergy. 1-3 They include penicillins, along with
cephalosporins, carbapenems, and monobactams. Most
reactions are benign T-cell mediated delayed exanthemas,
with SCARs being uncommon. 21 Life-threatening
anaphylaxis occurs approximately in 0.001% of cases
with parenteral exposure and even less for oral exposure.22
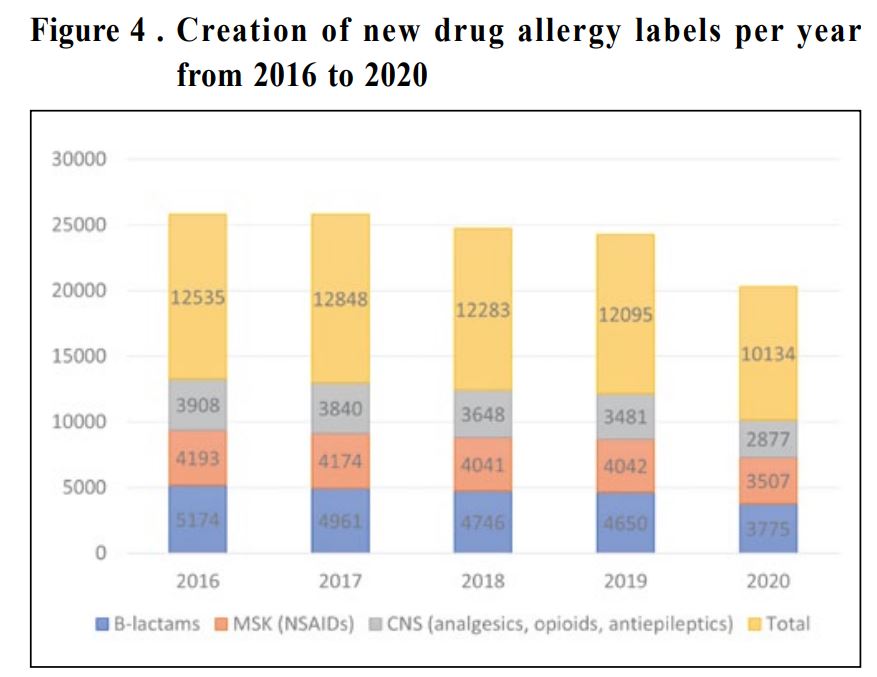
From 2016-2020, the majority of drug allergy
labels created have been due to labels. In 2020, the
point prevalence of BL antibiotic allergy labels was
2.0% and cumulative incidence of 107 per 100,000
population.23 (Figure 4) These findings mirror global
trends, with 5-15% patients labelled with penicillin
allergy in developed countries.
However, from our experience, many patients carry
“false” BL drug allergy labels that are unsubstantiated
by proper history or allergy testing. Following formal
allergological workup of BL allergies, we discovered
that less than 14% of patients labelled with BL “allergy”
were genuinely allergic.23,24 This high rate of inaccurate
labelling was similar to reports in western cohorts.25
Consequences of misdiagnosed allergiesThe detriment of allergy mislabels affects every branch of clinical medicine, with observable negative consequences on patients, healthcare systems and communities. (I) Effects on patients Patients with inappropriate allergy labels may be relegated to use alternative antibiotics with more side effects and lower efficacy, such as fluoroquinolones or vancomycin, even when BL antibiotics are indicated. This inadvertently increases the risk of adverse clinical events, such as increased hospital admission rates and length of stay, treatment costs, and deaths. While the effects of unnecessary allergy labels are apparent across all age-groups and conditions, they disproportionately affect high-risk patient groups.26 Geriatric patients with BL allergy labels have higher mortality rates and required more frequent transfers to convalescent or rehabilitation care centers.27 Furthermore, surgical patients with penicillin allergy labels are more likely to receive inferior perioperative prophylactic antibiotic choices, increasing the risk of postoperative infections by 50%. 28 Correcting false allergy labels can resume life-saving medications, reduce healthcare costs, and improve quality of life especially for high-risk patient groups. (II) Effects on healthcare system
How do we work up an antibiotic allergy?A comprehensive history is perhaps the most important part of evaluating any drug allergy. In our previous study, we identified that history of anaphylaxis and duration since the index reaction are important predictors of genuine allergy.24 Informative clinical histories can help in patient risk stratification, and in many cases, excludes the need for allergy testing. Some patients deemed at higher risk may undergo further evaluation, including skin testing and in-vitro tests. Drug provocation tests remain as the “gold standard” and are necessary to confidently confirm tolerance of BL.31,32 The diagnosis of a drug hypersensitivity is usually based on clinical judgement, and the general criteria can be considered under the following general framework:
Hong Kong Drug Alleregy Delabelling Initiative: - educate, outsource and empowerDespite extensive and devastating impacts of incorrect BL allergy labels, less than 1% of reported allergies are re-challenged through allergy evaluation per year globally, and 1 in 50 population of HK are waiting to be delabeled annually. Even with the formal establishment of Immunology & Allergy Services in Hong Kong, a lack of specialists and limitation in costs pose an unresolved challenge to comprehensive testing and delabelling. Multidisciplinary efforts across specialties, primary care and hospital settings, allied health professionals, and territory-wide clusters are critically needed. In response to this, the Hospital Authority’s HKWC piloted the territory’s Drug Allergy Delabelling Initiative (DADI) in 2019, following the establishment of the Penicillin Allergy Pathway (Figure 5) and Low-Risk Penicillin Allergy Clinic. 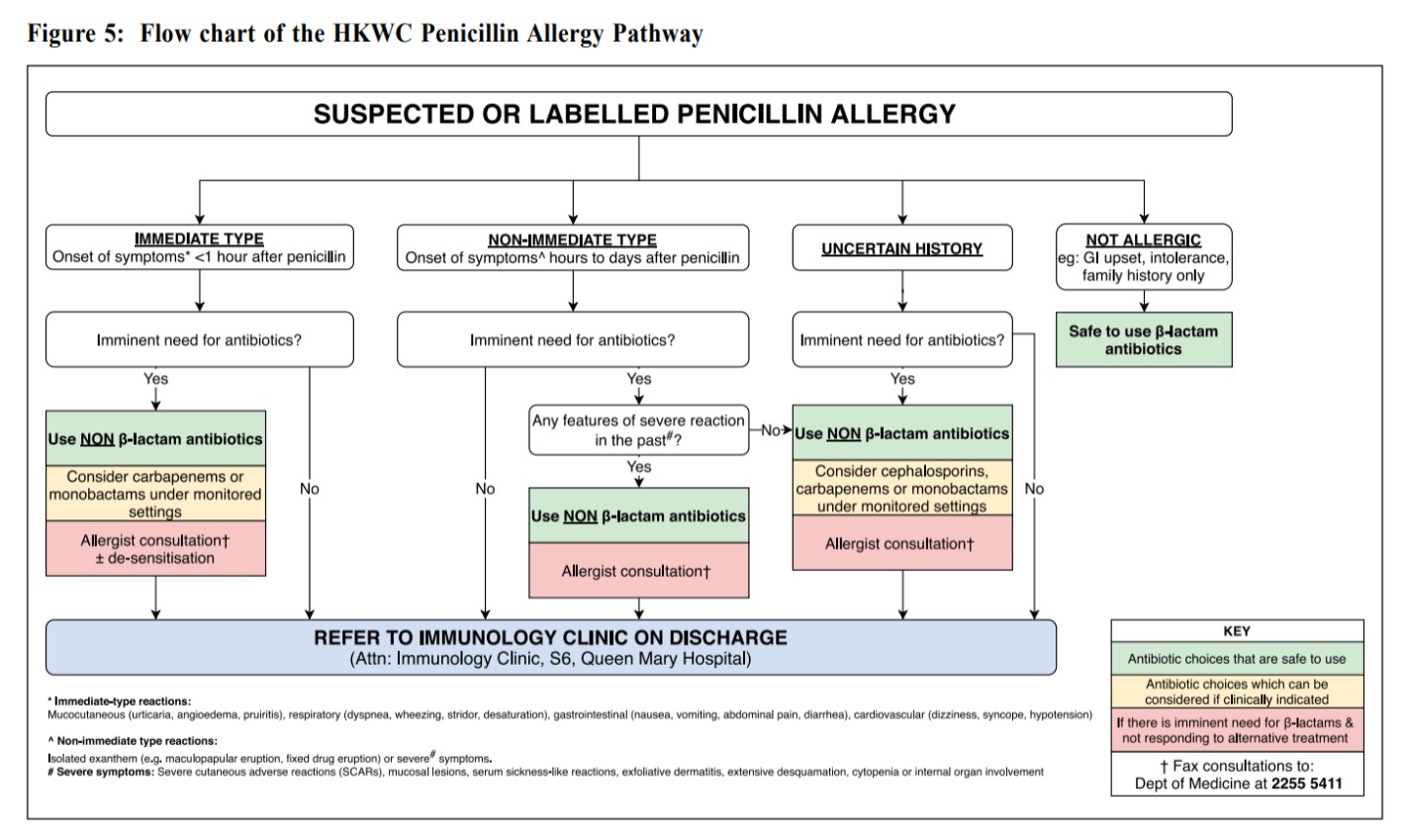
The HKWC Penicillin Allergy Pathway & Low- Risk Penicillin Allergy ClinicThe Penicillin Allergy Pathway is a simple infographic available to all in-patient wards of all hospitals under the HKWC. In addition to antibiotic suggestions during the patient's admission, all unclarified suspected BL allergies are referred to our Immunology Clinic for pro-active allergy delabelling. Patients triaged as low risk for genuine BL allergy are seen at our “fast track” dedicated Low-Risk Penicillin Allergy Clinic. This clinic maximizes the number of patients seen, resulting in 99% of allergy labels removed. Following the success of the Vaccine Allergy Safety Hub-and-Spoke clinics34, HK-DADI adopted its model for allergy delabelling services. HK-DADI is a protocol-driven, multidisciplinary model designed to tackle penicillin allergy by incorporating nurses and allied health professionals in allergy assessment.34 Patients referred to our Immunology Clinic for workup are first triaged by a nurse-led telephone interview. Those classified as “low-risk” then attend a Low Risk Clinic, where penicillin skin testing and provocation testing are performed by trained nursing professionals, supported by an overseeing physician. Following a negative provocation tests, the patients are counselled and given a detailed and personalised letter with their updated drug allergy record for their future medical reference. Our pilot study removed 90% of penicillin allergy labels from 312 attending patients. 
DADI has managed to shorten the waiting time for a routine penicillin allergy consultation from over 7 years to around 1 year. Our pilot analysis also showed a higher rate of future penicillin use following delabelling (compared with the traditional delabelling) and mitigated the need for unnecessary skin testing among low-risk patients. Recognising its success, the Hong Kong Hospital Authority plans to roll-out six additional HK-DADI pathways throughout all regional hospitals of Hong Kong in 2022. Our Hub-and-Spoke models aim to empower individual spokes and non-allergists to be able to provide service and foster more interest in allergy care. The central hub serves to provide training for other clusters, with multi-disciplinary collaborations with Infectious Disease specialists, pharmacists, and internists. Our success highlights the important role of Allied Health Professionals and the collaborative effort in patient management and care. References
Valerie Chiang,
MBBS (HK)
Maegan HY Yeung,
BA (Cantab)
Philip H Li,
MBBS (HK), MRes(Med) (HK), MRCP (UK), FRCP (Glasg)
Correspondence to: Dr. Philip H Li, Department of Medicine, Queen Mary Hospital, The
|
|