
|
June 2022,Volume 44, No.2
|
Discussion Paper
|
The role of family physicians in managing obesity in primary care settingWai-man Yeung 楊偉民,David VK Chao 周偉強 HK Pract 2022;44:52-58 SummaryObesity is a chronic health problem on the rising trend and affecting people globally and also those of Hong Kong. Its causes are multi-factorial and it is a major risk factor for several non-communicable diseases, resulting in significant morbidities and mortality. Most of these patients are managed in the primary care setting, and the interventions may include a combination of health advice, dietary control, physical activities, medications and surgery delivered by a multi-disciplinary team. The continual, comprehensive, coordinated and wholeperson care by the family physicians makes them the best position to care and manage the obesity patients. Keywords: Obesity, Family physicians, Primary care
摘要無論全球還是香港,肥胖都是一個呈上升趨勢的慢性健 康問題,它是由多種因素造成的。肥胖是幾種重要的非 傳染性疾病的主要危險因素,會造成患病率和死亡率的 明顯升高。 絕大部分的肥胖病人是在基層醫療就醫,肥胖的治療需 要多學科聯合進行,包括醫學健康指導,飲食管理,運 動, 藥物以及外科手術。由於家庭醫生的診治有持續 性,綜合性,協調性,而且是全人醫療,令家庭醫生成 為治療肥胖患者的最佳人選。 關鍵詞: 肥胖,家庭醫生,基層醫療 IntroductionObesity is a health problem often encountered by the practising family physicians, and involves patients of all ages, male or female. Though common, its management is challenging owing to its chronic nature, as it may affect the patients’ physical, psychological and social wellbeing, resulting in significant morbidities and mortality. The treatment may involve collaborations across several healthcare disciplines requiring good coordination of care by the family physician. On the other hand, obesity is preventable especially if the relevant issues could be addressed from early on in life. This article aims to provide updated information on obesity management to the busy family physicians who would like to provide better care for patients suffering from obesity. EpidemiologyAccording to the World Health Organisation (WHO) in 2021, worldwide obesity has nearly tripled since 1975. In 2016, over 1.9 billion adults (39%) were overweight, including over 650 million (13%) who were obese. Most of the world's population lives in countries where overweight and obesity kill more people than underweight related issues do. In 2016, over 340 million children and adolescents aged 5-19 were overweight or obese. In 2020, 39 million children under the age of 5 were overweight or obese.1 In Hong Kong, according to the Population Health Survey (PHS) 2014/15 conducted by the Department of Health, 29.9% (24.4% of females and 36.0% of males) of population aged 15-84 were obese, with another 20.1% (19.3% of females and 20.9% of males) being overweight. Obesity was most common among females aged 65-84 (34.3%) and males aged 45-54 (51.1%).2 What is Obesity?“Overweight and obesity are defined as abnormal or excessive fat accumulation that may impair health.”1 Several methods can be used to measure body fat, each with its strengths and limitations, such as just simply using the body weight, or the body mass index (BMI), waist circumference, waist-to-hip ratio, weight-toheight ratio, skinfold thickness, bioelectrical impedance, or the more sophisticated tests including magnetic resonance imaging (MRI) and the dual energy X-ray absorptiometry (DEXA).3,4 Among these methods, BMI provides the most convenient population-level measure of overweight and obesity as it is the same for both sexes and for all ages of adults.1 It is defined as a person's weight in kilograms divided by the square of his height in metres (kg/m2). However, it should be considered as a rough guide only because it cannot be used to differentiate between fat and lean muscle weight, and may not correspond to the same degree of adiposity in different individuals. BMI may be a less accurate measure in highly muscular adults and should be interpreted with caution in this group.1,3,4,5 Nonetheless, with its simplicity and practicability, BMI provides a useful means to assess adult patients’ obesity in a family physician’s office. For children, age needs to be considered when defining overweight and obesity. The classification between normal, over-weight and obesity with BMI is shown in Table 1. Apart from BMI, waist circumference is also recommended as an adjunctive measurement for obesity in people with BMI less than 35 kg/m2. However, for children, waist circumference is not recommended as a routine. Bioimpedance is not recommended as a substitute for BMI to measure adiposity.5 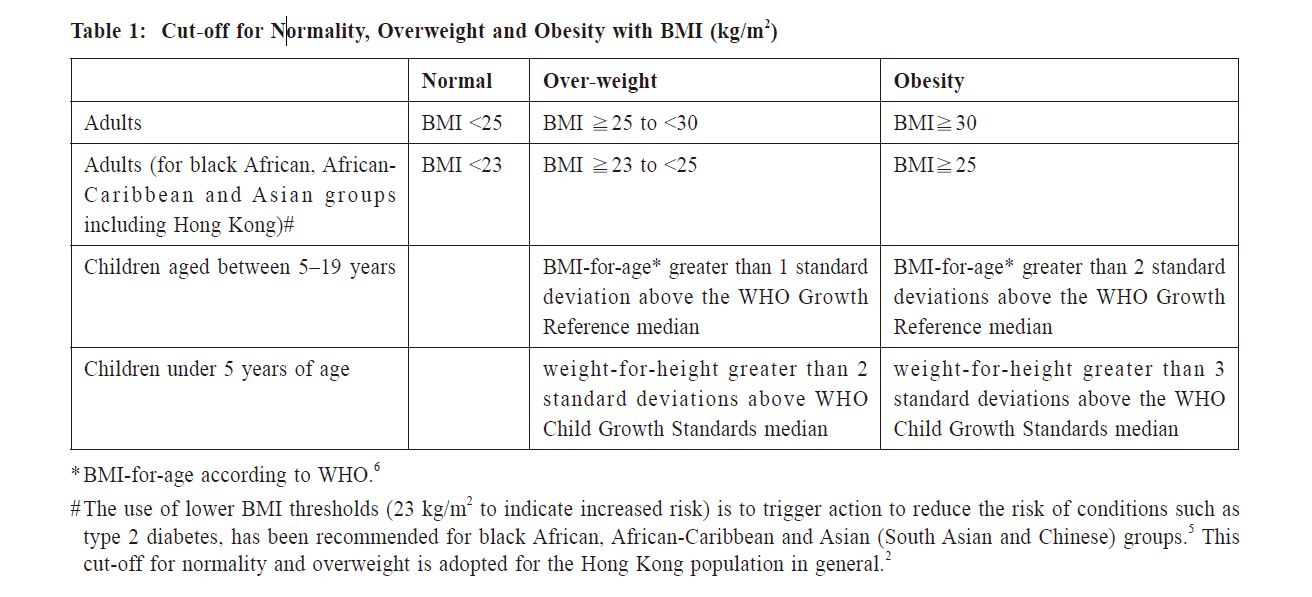
Causes of ObesityMost obesity and being overweight result from an energy imbalance between calories consumed and calories expended. Worldwide, there has been an increased intake of energy-dense diet rich in fat and sugars, and a decrease in physical activities due to the increasingly sedentary work nature, changing modes of transportation, and increasing urbanisation.1 The underlying causes of obesity can be more complex and are multifactorial, and include epigenetics and alteration in the gut microbiome. Although the heritability of obesity has been shown in twin studies, only a minority of patients have a purely genetic cause (e.g. leptin deficiency), and not many patients have a purely medical cause of obesity (e.g. hypothalamic tumour). Socio-economic factors also play a part in facilitating weight gain. Mental health issues can lead to obesity. Weight gain may be a result of impaired motivation or self-care, insomnia, inactivity or unhealthy relationships with food. Besides, obesity can be the side effects of many psychotropic medications.7 Consequences of ObesityRaised BMI is a major risk factor for several noncommunicable diseases (see Table 2). Weight reduction will be beneficial for obese patients to reduce their risk of developing these complications. In particular, in patients with BMI>35 kg/m2, these co-morbidities are likely to be present, and a greater than 15-20% weight loss, which will always be over 10 kg, will be required for these people to obtain a sustained improvement in co-morbidity.8 Obese children may have breathing difficulties, increased risk of fractures, hypertension, early markers of cardiovascular disease, insulin resistance and psychological impairments. They will also have a higher chance of obesity,premature death and disability in their adulthood.1 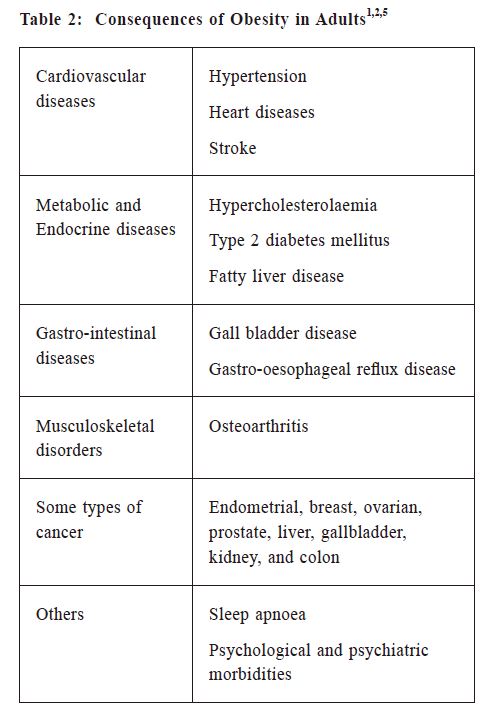
Management of ObesityIdentification Early identification of the overweight or obese patients in our practice by measuring their BMI is desirable, such that intervention can be started early. Opportunity screening can be done at the time of registration in the practice, consultation for related conditions (such as diabetes and hypertension) or other routine health checks.5,9 Initial AssessmentThis covers a wide scope covering the physical and psychosocial dimensions of the patients, and includes that of obesity itself, the possible underlying causes and the co-morbidities which should be managed once identified. Risk factors are to be assessed by measuring the blood pressure, lipid profile and HbA1c. Family history of obesity or metabolic diseases, lifestyle, exercise, dietary issues, occupational history, and drug history are also important. For children, growth and puberty status should be examined, and assessment of co-morbidity (such as hypertension, hyperinsulinaemia, dyslipidaemia, type 2 diabetes, psychosocial dysfunction and exacerbation of conditions such as asthma) should be considered with a BMI at or above the 98th centile. Consider referral to a paediatric specialist for children who have significant co-morbidities (e.g. benign intracranial hypertension, sleep apnoea, obesity hypoventilation syndrome, orthopaedic problems) or complex needs (e.g., learning disabilities). The assessment for these children may include blood pressure measurements, lipid profile, fasting insulin, fasting glucose and oral glucose tolerance test, liver function and endocrine function.5,8 Psychosocial distress or any environmental factors which are obstacles for weight reduction should be looked for. In children, it can present as low selfesteem, teasing and bullying. The role of family and carers in supporting patients, to make lifestyle changes is part of the assessment.5 The patients’ beliefs, attitude and behaviour will influence the progress of the intervention and can be assessed by what is shown in Table 3. If the patients or their family feel this is not the right time to intervene, we can provide our contact details and offer that advice and support will be available in the future whenever they want it. Interventions for Obese PatientsSeveral guidelines suggest different levels of intervention, from general advice on healthy weight and lifestyle, to diet, physical activities, medications, surgery, and given as different combinations of these options, by a multi-disciplinary team (including the family physicians, nurses, dietitians, physiotherapist, pharmacists, clinical psychologist, bariatric surgeons and social workers).5,8,9,10 The level of intervention should be higher for patients with co-morbidities. Stratified plans can be applied according to the patient’s BMI +/- waist circumference5, with flexibility according to local practice experience. 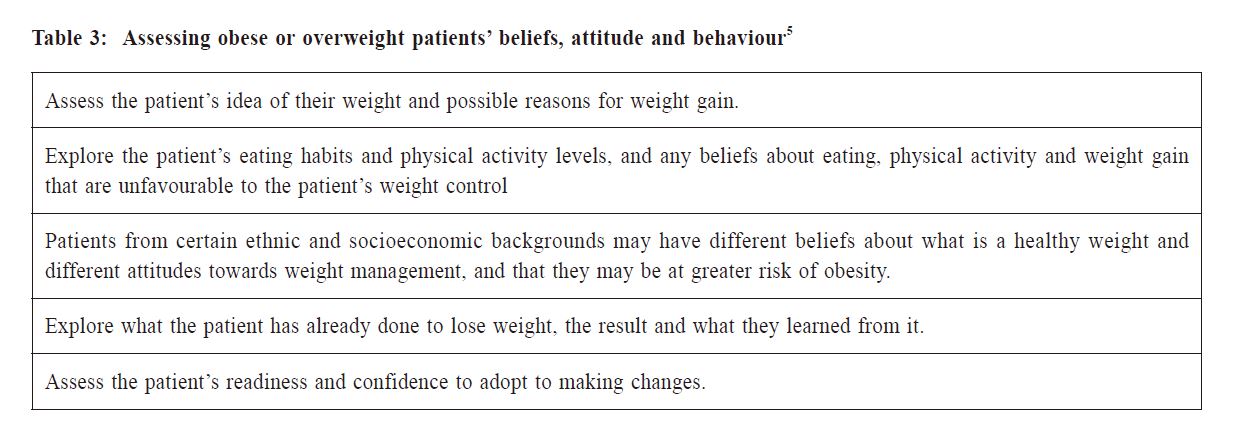
General PrinciplesAs a start, offer patients simple advice and relevant information about the benefits of losing weight if they are ready to talk about it. It should be stressed that overweight and obesity, as well as their co-morbidities, could be preventable. Offer regular, long-term followup and support to the patients. Good record keeping is necessary to ensure continuity of care. It has been recommended that “supportive environments and communities are fundamental in shaping people’s choices, by making the choice of healthier foods and regular physical activity the easiest choice (see Figure 1), and therefore preventing overweight and obesity”.1 To echo with this, it has also been reported that using a single dietary adjustment may produce weight loss similar to more complex plans. For example, encouraging a patient to increase dietary fiber intake produces comparable adherence and weight loss to encouraging compliance with the multiple goals of the American Heart Association diet.9 Simple plan works and is more acceptable to patients. 
For children and young people, it is necessary to coordinate their care according to their individual and family needs, the decisions of any interventions made with them, to the feasibility within their social settings, and a supportive environment which promotes lifestyle changes to be created. This “environment” can be somewhere other than home such as schools. Parents should be encouraged to take the main responsibility for the child’s lifestyle changes, taken into considerations the age and maturity of the child. Another point to be noted is that child abuse can be a contributory factor to or a cause of obesity in children. Abuse may also coexist with obesity.5 Be sensitive to patients’ needs when giving advice because of their different cultural backgrounds and ethnicities, such as the choice of food. Health information in the form of pamphlets or electronic version can be offered to patients. It is worthwhile to explain to the patients that the change from losing weight to maintenance typically happens after 6 to 9 months of treatment. Set realistic targets for weight loss and praise successes at every opportunity to encourage the patient through the difficult process of changing established behaviours. For children and young people, the focus may be weight loss or just weight maintenance depending on the person’s age and stage of growth. If their parents are also obese, they can be invited to manage their own weight alongside with their children too. For any patients, engage their relatives to support any weight management programme.5 DietPatients can be advised to limit intake of energydense foods; and to increase consumption of low energydense foods (fruit, vegetables, legumes, whole grains and nuts).1,8 Tailor dietary changes to food preferences. Unduly use of restrictive and nutritionally unbalanced diets is not recommended, because they are ineffective in the long term and can be harmful. For adults, the dietary approach to weight loss is that total energy intake should be less than energy expenditure. Diets that have a 600 kcal/day energy deficit (i.e., they contain 600 kcal less than the person needs to stay the same weight) or that reduce calories by lowering the fat content (low-fat diets), in combination with expert support and intensive follow up, are recommended for sustainable weight loss.5 Low-calorie diets (800–1600 kcal/day) can be considered but these are less likely to be nutritionally complete. Very-low-calorie diets (800 kcal/day or less) are usually not used except for obese people with a clinically-assessed need to rapidly lose weight (for example, people who need joint replacement surgery or who are seeking fertility services). People should be encouraged to eat a balanced diet in the long term.5,8 For children, any dietary recommendation should be part of a multi-component intervention. A dietary approach alone is not recommended. Any dietary changes should be age appropriate. For overweight and obese children and young people, total energy intake should be below their energy expenditure.5 Patients of any ages can be referred to dietitian if needed. Physical ActivitiesOverweight and obese individuals should be prescribed a volume of physical activity equal to approximately 1,800-2,500 kcal/week. This corresponds to approximately 225-300 min/week, or about 45 to 60 minutes per day of moderate intensity physical activity, particularly if they do not reduce their energy intake. For those who have been obese and have lost weight, they may need to do 60 to 90 minutes of activity a day to avoid regaining weight. Choices of physical activities may include activities that can be incorporated into everyday life, such as brisk walking, gardening or cycling, supervised exercise programmes, other activities such as swimming, aiming to walk a certain number of steps each day, or stair climbing. The patients’ current physical fitness should be taken into account. Children and young people should be encouraged to increase their level of physical activity, with the choice of activity appropriate to the child's ability and confidence. Even for children without the need to lose weight, exercise will still be beneficial (for example, reduced risk of type 2 diabetes and cardiovascular disease). Children who are overweight may need to do more than 60 minutes' activity. Encourage people, adults or children, to reduce the amount of time they spend inactive, such as watching television, using a computer or playing video games.5,8,9 Drug TreatmentPharmacological treatment should only be considered after dietary, exercise and behavioural approaches have not brought about the targeted weight reduction. The decision to start drug treatments should only be made after discussion with the patient on the potential benefits and limitations, the mode of action, adverse effects and monitoring requirements, and the potential impact on the person's motivation. When drug is prescribed, the patient should still be supported and counselled on additional diet, physical activity and behavioural strategies. Orlistat is an adjunct to lifestyle interventions in weight reduction management, and could be considered as part of an overall plan for managing obesity in adults with a BMI ≧ 28 kg/m2 with associated risk factors, or a BMI ≧ 30 kg/m2.5,8,9 It should only be continued beyond 3 months if the person has lost at least 5% of their initial body weight since starting drug treatment. The use of drug treatment for longer than 12 months (usually for weight maintenance) should only be decided after discussing potential benefits and limitations with the patient thoroughly. The co-prescribing of orlistat with other weight reduction drugs is not currently recommended. If micronutrient deficiency is a concern, a supplement providing the reference nutrient intake for all vitamins and minerals should be considered, particularly for older people who may be at risk of malnutrition, and young people who are in their growth and development. Rates of weight loss may be slower in type 2 diabetic patients, so less strict goals may be more appropriate for them. Other medications for longterm treatment of obesity include lorcaserin, liraglutide, phentermine/topiramate, and naltrexone/bupropion.9 On the other hand, drug treatment is not generally recommended for children except for those with comorbidities such as orthopaedic problems, sleep apnoea or severe psychological co-morbidities, and prescribing should be started and monitored only in paediatric specialist settings.5
Bariatric SurgeryThis includes gastric banding, gastric bypass, sleeve gastrectomy and duodenal switch, and is usually undertaken laparoscopically. Bariatric surgery is a treatment option for people with obesity. Similar to BMI with different cut-off values for obesity, there are also different criteria for using bariatric surgery for treating obesity in different parts of the world. In Hong Kong, according to the Hospital Authority’s Guidelines on Metabolic & Bariatric Surgery for Severely Obese Adult Patients, bariatric surgery is primarily aimed for weight loss in patients with severe obesity and failed weight loss after attempts of lifestyle and dietary modification +/- pharmacological therapy, and is indicated for patients with BMI ≥ 35kg/m2 in Asian (or BMI ≥ 40kg/m2 in Caucasian) with or without co-morbidity, or BMI ≥ 30kg/m2 in Asian (or BMI ≥ 35kg/m2 in Caucasian) with significant obesity-related co-morbidity as listed in Table 4. Surgical intervention is not generally recommended in children or young people.5,9,11After the surgery, a greater emphasis should be placed on support and follow up, and also with clear postoperative dietary advice for risk of significant metabolic chang (e.g., vitamin B12 and iron deficiency). It has been suggested that resolution of type 2 diabetes may be an additional outcome of surgical treatment of morbid obesity. It has been estimated that about 60% of patients with type 2 diabetes achieve remission after Roux‑en‑Y gastric bypass surgery. It has also been suggested that diabetes-related morbidity and mortality is significantly lower after bariatric surgery and that the improvement in diabetic control is longlasting.5 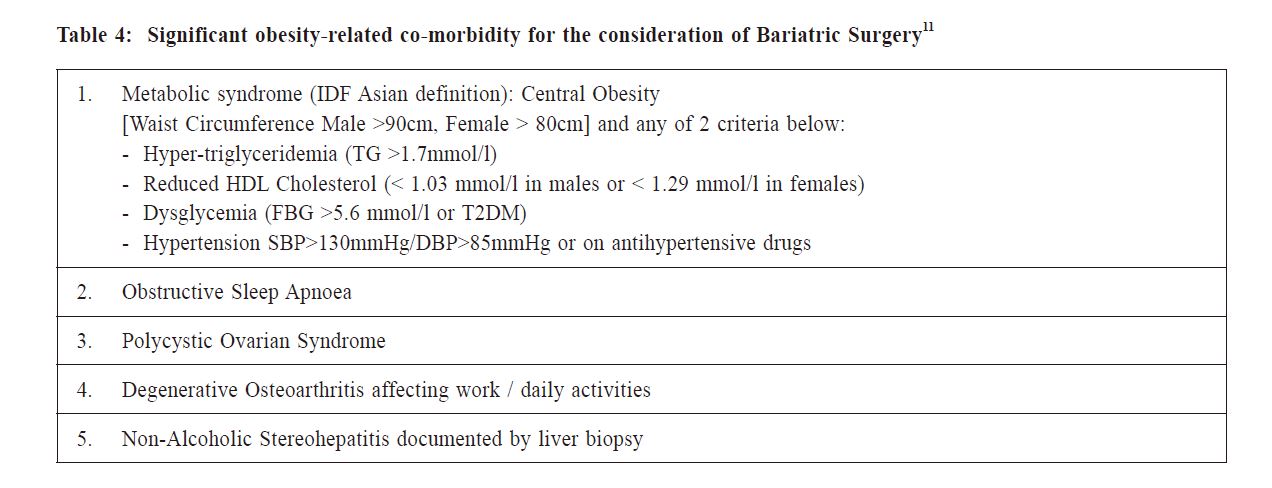
Roles of the Family PhysiciansObesity is a commonly encountered problem in the primary care setting. In the author’s opinion, its management may be further enhanced even during a busy clinic or the patients being still in precontemplation of change. In view of the large number of obese patients in our population, a well-trained primary care workforce is essential to work on the prevention and management of this problem. Family medicine is a fundamental component of primary care, and family physicians are “in a unique position to bridge issues that cross primary care and public health”, as they “deal with individuals day to day, but also have a deeper understanding of the communities in which they work”.7The identification, assessment and interventions for obese patients have been discussed above. These can be integrated as a coordinated and comprehensive healthcare plan, and are within the scope of services provided by the family physicians. Health education on a healthy lifestyle with dietary control and physical activities for the general public should also be the basis of obesity prevention in our society. However, despite all the evidence of the best care for obese patients, the success of these interventions could be hindered by the patients’ non-acceptance, noncompliance and non-adherence with these management plans. These patients may have different reactions to their health situation, such as denial, anger or disbelief, and that may diminish their ability or willingness to change their lifestyle. The family doctors, with their training in whole person care, and also with their continual and long term relationship with their patients, should be in the best position to help these patients by being their health navigators. A family doctor should be sensitive enough to acknowledge the difficulties faced by the obese patient, and be able to show empathy which will lead to more open discussion. The doctor can explain to the patients that obesity is a clinical term with specific health implications, rather than a question of how people look; this may reduce any potential negative or stereotyped feelings in the patients.5 Public messages on obesity that focus mainly on body weight contribute to stigma and bias. Instead, the emphasis should be changed from “loss of weight” to “gain in health”.7 Hong Kong people in general are very busy and often under stress, and many people have difficulty finding the time for exercise and to eat healthily. Apart from providing information and advice, an important role of the family doctors is to show their support and concern to their patients, and in the author’s opinion, it is something the patients need and will appreciate. The path for weight reduction takes time and is not easy, and patients need someone as a companion to give them strength and hope, and also to help them to persevere. The final success will be rewarding to both the patients and their doctors. 
ConclusionWe are now in a crisis of seeing too many obese people, including our children who will be the future of our society. Apart from the hard work of the family doctors, we also need the participation of other parties who can take a part in the control of obesity in our population. We want our next generation to be a healthier one, and solving the issue of childhood obesity requires multiple parties to act in synergy – the health sector, the government, the food industry, families and of course, parents.12 As final words, managing obesity is something of importance in our society and the success of which will rely on the appropriate utilisation of clinical expertise, a multi-disciplinary healthcare team led by the family physicians, and the collaboration of different stakeholders in the community.References
Wai-man Yeung,
MBBS(HK), FRCSEd, FRACGP, FHKAM (Family Medicine)
David VK Chao,
MBChB (Liverpool), MFM (Monash), FRCGP, FHKAM (Family Medicine)
Correspondence to:
Dr Wai-man Yeung, Associate Consultant, Shau Kei Wan Jockey
|
|