
|
March 2022,Volume 44, No.1
|
Original Article
|
Nurses’ attitude to seasonal influenza vaccination in primary care outpatient clinics: a qualitative studySharon SW Ho 何書韻,Yeung-shing Ng 吳楊城,Tsun-kit Chu 朱晉傑,Phyllis Lau 廖明玉,Jun Liang 梁峻 HK Pract 2022;44:3-10 Summary
Objective:
To explore the attitude of nurses towards
seasonal influenza vaccination (SIV) in primary care
outpatient clinics in Hong Kong
摘要
目的 :
探討香港基層醫療門診護士對季節性流感疫苗的態度。
關鍵詞 : 態度,護士,流感,疫苗接種,質性研究 IntroductionThe importance of receiving seasonal influenza vaccination (SIV) amongst health care professionals (HCPs) is substantial. HCPs are exposed to patients with influenza in the workplace, being at risk of occupationally-acquired influenza, and of transmitting influenza to patients and other healthcare practitioners. HCPs belong to high-risk groups for contracting influenza, and is therefore prioritised for SIV.1,2 A study in a hospital in Italy found that in influenza epidemic period, absenteeism increased by 65% (from 4.05 to 6.68 days/ healthcare worker).3 Randomised controlled studies demonstrated that a high rate of SIV among HCPs could significantly reduce mortality and influenza-like illness in hospitals and long-term care facilities.4,5 A Cochrane review showed that HCPs vaccination could reduce influenza infection by 52% and all-cause mortality by 55%.6 Despite the clear demonstrable benefit of SIV in the scientific literature, it is still controversial as to whether SIV should be mandatorily administered to HCPs. Policy makers and healthcare managers need to strike a balance between scientific evidence of SIV, public values of the community, professional ethics and personal liberty of HCPs.7 It is also necessary to understand why a proportion of HCPs refused SIV. Research studies have been conducted to explore the barriers and facilitators of SIV uptake among HCPs. In 2009, a systematic review on attitudes and predictors of influenza vaccination in HCPs found 2 major barriers: (1) misconceptions or lack of knowledge about influenza infection, (2) lack of convenient access to vaccination. On the other hand, idea of self-protection was the most important reason of receiving vaccination.8 In 2017, a systematic review of 25 qualitative studies on SIV acceptance among HCPs found a variety of beliefs serving as barriers, including concerns about side-effects, skepticism about vaccine effectiveness, and the belief that influenza is not a serious illness.9 It is clear that promotion of SIV should take into account both the individual beliefs of the targeted HCPs and the organisational context within which they are implemented. None of the studies included in these two reviews were conducted in Hong Kong. Our local data showed that the SIV coverage rates in 2016/2017 in different healthcare disciplines were 44% for medical, 39.6% for supporting, 26.2% for allied health, and 24.5% for nursing staff in Hospital Authority.10 Similar patterns of different coverage rate in different disciplines were also found in overseas studies.11,12 One local survey reported that the SIV coverage rates in nurses have fallen from 57% in 2005 to 24% in 2012.13 The declining SIV coverage among nurses is a public health concern. In fact, healthcare managers should take efforts to improve the SIV coverage in healthcare providers of all levels and disciplines, and nurses are no exception. Primary care nurses are instrumental in providing direct contact with the general public for promoting and administrating SIV.14 Previous studies also showed that nurses who had received SIV are more effective in influencing the general public in receiving the SIV.15 Based on the finding of previous local studies 16 we aimed to re-visit this important topic by conducting a qualitative study on nurses’ attitudes towards SIV programme in Hong Kong. Our objective was to identify additional useful information regarding the facilitators and barriers of SIV among the nursing profession. These qualitative data may be useful for future development of more effective SIV programmes. MethodsA) Study design This study adopted a qualitative phenomenological approach to examine the SIV coverage among nurses. In-depth, semi-structured interviews were conducted to explore individual participant’s views and beliefs regarding vaccine facilitators, barriers and other heuristic factors towards SIV. The Health Belief Model (HBM)17 was used to develop the interview questions. The six constructs of HBM include: (1) perceived susceptibility (the likelihood of getting a disease), (2) perceived severity (feelings about the seriousness of contracting an illness or of leaving it untreated), (3) perceived benefit (beliefs regarding perceived benefits of various available actions for reducing the disease threat), (4) perceived barrier (the perceived potential negative aspects of a particular health action), (5) cues to action (cues that can trigger actions, such as bodily event, e.g. an illness, or environmental events e.g. media publicity), and (6) self-efficacy (the conviction that one can successfully execute the behaviour required to produce the outcomes).18 B) Outcome measurements The outcome measurement are: ( 1 ) demographics, such as gender, age, rank and duration of nursing experience, (2) perceived susceptibility to influenza, (3) perceived severity and consequence of acquiring influenza, (4) vaccination status in 2018/2019 SIV programme, and the perceived effectiveness of SIV, (5) perceived risks of having SIV (and the source of information), (6) obstacles and prompts of SIV provision, (7) personal views on SIV programmes, including mandatory SIV, declination forms and incentives for SIV. C) Subjects Nurses were recruited from 11 primary care outpatient clinics in the Department of Family Medicine &Primary Health Care, the New Territories West Cluster. (Within the Hospital Authority of Hong Kong, hospitals and clinics are organised into seven clusters based on their locations.) Purposive sampling was employed to maximise the variation in age, work experience and rank. The inclusion criteria were: (1) nurses aged between 18 and 65 years old and (2) being able to communicate in Cantonese. Nurses who could not speak in Cantonese were excluded. The study objective was explained to the participants. Written consent had been obtained before interview and intention for findings check and transcript return was enquired. D) Data collection One-to-one interviews were conducted in Cantonese from March to April 2019 at the clinics where the participants worked. Interviews were conducted in a quiet room to ensure confidentiality: interviews were conducted in a soundproof room with curtains, any third party was prohibited to gain access to the interview room during interview. Also the interview materials were kept confidential by the primary investigator. Interviews were audiorecorded and transcribed verbatim. Field notes were taken with permission. Transcripts and field notes were de-identified using pseudonyms. We continued to conduct more interviews until thematic saturation has been reached. We found that after 20 interviews, the themes have repeated and saturated, without additional information collected. E) Data analysis Each transcript was checked against the audio-records and field notes for accuracy. A pre-determined flat coding frame based on the variables from HBM was developed. Transcripts were analysed and coded using key words and phrases in the frame using line-by-line deductive coding. Coding started soon after interviews were conducted. Notes were made throughout the analysis. All transcripts were coded by one team member, and two transcripts were selected for second coding by another team member. Codes were then grouped into themes following further discussion with the team. Consensus was reached after discussion and agreement among team members. Referral to a third party for final decision would be made if consensus cannot be reached. Findings were illustrated with representative quotes, which were translated into English. Quotes were selected for back translation and were examined for consistency. F) Ethics approval This study was approved by Research Ethics Committee of the New Territories West Cluster, Hospital Authority of Hong Kong. (Ref.:NTWC/ REC/18079 dated 6/11/2018) G) Results - 1) Perceived susceptibity and seriusness of disease, 2) effectiveness and risk of, 3) provision of, and 4) methods of provision of vaccination A total of twenty nurses were interviewed (19 female). Seven (35%) received SIV in year 2018/19. Their work experience ranged from 0.5 to 30 years (average = 9.5 years). The sample comprised five advanced practice nurses, twelve registered nurses and three enrolled nurses. 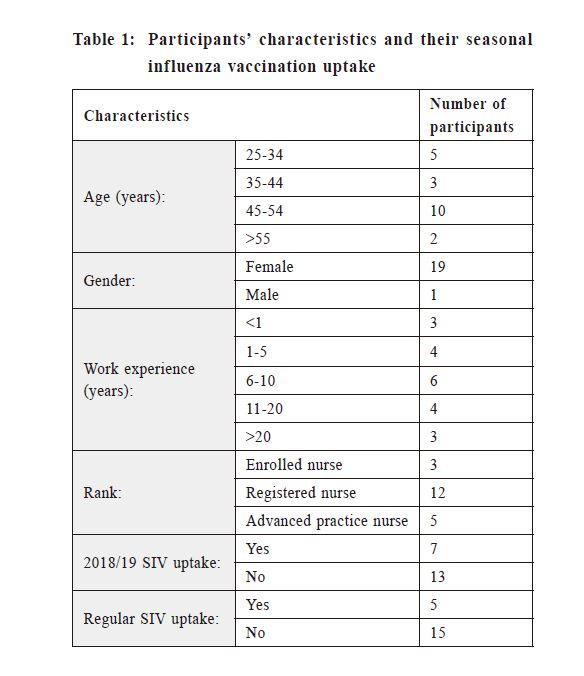 1. Perceived susceptibility and seriousness of influenzaIn both vaccinated and unvaccinated nurses, the majority regarded themselves as susceptible to influenza (6/7 in the vaccinated group, 11/13 in the unvaccinated group). The reasons were workplace exposure to high-risk patients and patients with influenza-like illnesses. Both groups acknowledged that influenza can be a serious illness which might lead to complications and mortality. They regarded seriousness as a significant variable among individuals. “Reaction to influenza differs among individuals; it’s more serious in the physically weak.” (Unvaccinated L) Unvaccinated nurses mentioned more about their own advantageous characteristics (e.g. not at extreme age, strong immunity, acquired immunity from past infection) and taken actions (e.g. healthy lifestyle, personal hygiene) which reduced their susceptibility and counter-acted the seriousness. These were considered as alternatives to SIV with comparable or non-inferior effectiveness. “Every year soon before the start of SIV campaign, I fell sick. Once I have fallen ill, I won’t get sick again.” (Unvaccinated G) “Although I am susceptible, it’ll be okay as long as I follow the preventive routines at work, e.g. hand washing, wearing mask.” (Unvaccinated C) 2. Perceived effectiveness and risks of SIVa) Parceived effectiveness Both the vaccinated (6/7) and unvaccinated nurses (11/13) regarded SIV as effective, but the degree of confidence and the basis of such confidence differed. Most (5/7) vaccinated nurses confidently believed in the effectiveness of SIV, based on their own past positive experience with SIV. “SIV was very effective. I didn’t get influenza after the vaccination. . In the year that I did not get vaccinated I fell ill with influenza. So I get vaccinated every year after I have resumed my job in these few years.” (Vaccinated D) In the unvaccinated group, most of them (10/13) acknowledged the statement that SIV was effective, but they had more reservations with regards to how effective it was. Their belief was mainly projected from information they have heard and “second-hand” experience about SIV. “If it (SIV) was useless, the Government wouldn’t have promoted it with so much effort. Therefore, I think it must have some benefit.” (Unvaccinated B) “I’ve seen the benefits in my family members and people around me. My mother-in- law, in her eighties, was prone A few unvaccinated nurses did not endorse SIV effectiveness, because the vaccine does not give protection against all strains of the influenza virus. “It really depends on whether the vaccination “hits” the target. Every year, the vaccine only selects 3 or 4 strains.” (Unvaccinated E) b) Perceived risk of seasonal influenza vaccination All the vaccinated nurses and many (9/13) unvaccinated nurses regarded SIV as safe. Knowledge was obtained from work-related education. Unvaccinated nurses had negative attitude towards SIV, attributing non-specific bodily discomfort or concomitant condition to SIV, despite acknowledgement of their safety. “A patient returned to clinic, two hours after vaccination; I noticed he presented with subconjunctival haemorrhage. I am not sure if it is related. (Unvaccinated I) Some unvaccinated nurses expressed fear over vaccine side-effect, such as Guillain- Barré syndrome, loss of function due to serious complication, and allergy. c) Seasonal influnza vaccionation provision Most nurses appreciated the free and prioritised SIV provision in place in the workplace and regarded it logistically friendly. However, concerns on annual administration managerial expectation and data privacy existed: “Some colleagues felt that disclosure of personal data was an obstacle to SIV. If their personal information was not exposed, they would have been more motivated.” (Vaccinated P) Existing SIV prompts included education, promotions on media, posters, mobile SIV teams, and senior role modelling etc. Most welcomed these measures, but these would not change their decision on vaccine uptake. d) Views on provision – i) mandatory SIV, ii) declination form, and iii) means of adding incentives i) Mandatory vaccination All but one participant opposed mandatory SIV. It was regarded as a violation of rights and autonomy. Fear of extending mandatory policy to other vaccines existed. Opinion on the ethical discussion of vaccination in the nursing profession was diverse. Some saw this as the nursing professionals’ responsibility for patient-protection, while some opined that it was asking too much of them. “Everyone has freedom of choice…… Mandatory SIV triggers rejection. I am all along accepting SIV. But if it’s made mandatory, I would say no.” (Vaccinated O) “Being a nurse is my job, but I won’t compromise on everything (SIV uptake) for being a nurse.” (Unvaccinated L) ii) SIV declining form Less than half of the nurses (8/20) accepted declination form. Some regarded the form as a tool to understand the reasons for declination, while others doubted if the respondents would give the sincere answer. “It can clarify the reasons for declination among colleagues, then work on them for better SIV promotion next year.” (Unvaccinated F) “Colleagues would fill the form, but the answers may not be true.” (Vaccinated R) iii) Means of adding incentive: Most nurses welcomed material rewards. However, they saw it as a boost to morale, rather than incentives which can affect their decision. Some volunteered the key determinants for their SIV decision, namely new positive experience with SIV, having their concerns fully addressed, convincing scientific evidence on effectiveness and safety of SIV, peer influence and a workplace culture to receive SIV: “Previously my perception of SIV was that of it could cause marked adverse reaction and severe pain. People think SIV is bad because of misunderstanding or past experience.” (Vaccinated P) “Nurses are peer-driven; we tend to get the jab if our peers do. It is impossible to do it for $100” (Vaccinated A) DiscussionRegarding the appraised threat of influenza, both the vaccinated and unvaccinated nurses agreed that they are susceptible, due to workplace exposure, and that influenza infection can be serious, with seriousness variable for individuals. However, the unvaccinated nurses believe more in the benefit of other actions, such as maintaining good general health and immunity which can effectively mitigate their own susceptibility and seriousness of infection. Regarding the perceived benefits and risks of SIV, both the vaccinated and unvaccinated nurses acknowledged the effectiveness of SIV, and that serious side effects were perceived as being very rare. This is different from other studies which suggested that side effects were the main barrier for SIV uptake.19-23 In the vaccinated nurses, their level of confidence in the effectiveness of SIV is higher, and their level of fear over the potential side effect is lower. The key motivating factor for vaccination is a strong belief on effectiveness of vaccination. This finding in the vaccinated group correlated with the finding of a local study on nursing students that perceived effectiveness facilitates vaccination uptake.19 The basis of personal belief on vaccine effectiveness appears to determine the level of confidence. In the vaccinated nurses, their belief on SIV effectiveness was based on personal positive experience with vaccination. The unvaccinated nurses have more reservation on the effectiveness, and their belief on vaccine effectiveness was based on scientific information they acquired through educ a t ion and s e cond-hand expe r i enc e (observing others, such as family, peers and patients), rather than personal positive experience of vaccination. The major factor deterring vaccination is a strong belief on alternative measures, apart from vaccination, in influenza prevention. This finding echoed a meta-analysis which found that a “healthy immune system” was seen by those who refused SIV as the most effective way to prevent influenza.24 Another deterring factor is bigger fear on the potential side effects. Some unvaccinated nurses attributed non-specific body discomfort to sequelae of vaccination, although they know these are not the known side effects of SIV. This apparent paradox might indicate a self-fulfilling prophecy in which people try to reduce the discrepancy between their behaviours (not vaccinated) and beliefs (serious-side effects are statistically very rare) in order to avoid the discomfort of cognitive dissonance.25 All participants agreed that the current SIV provision at workplace was practically barrier-free. Nearly all nurses objected to the notion of mandatory SIV campaign which is hence expected to be counterproductive. When the uptake rate is suboptimal and vaccination among healthcare workers is important for patient protection, mandatory vaccination, (i.e. making it a condition of employment,) appears to be a promising and well-justified policy. However, a study found that despite the good intention, mandatory SIV might give a perception that this was driven by an agenda of increasing productivity, not for healthcare workers’ own wellbeing.9 A qualitative study explored why nurses declined influenza vaccine found one major theme: a wish to have decisional autonomy - especially over one’s body and health.23 There is much doubt on the usefulness of declining form in exploring nurses’ reasons for having a declining SIV. Material rewards were welcomed but would be ineffective to increase uptake. This finding was in contrast to an oversea survey which found external motivation through rewards improving vaccination rates.26 Three findings in this study might shed light on what can be done differently in SIV campaign. First, some nurses expressed concern with regards to their personal data privacy, when receiving SIV in the workplace. Therefore, it might be helpful to review the moment when a nurse registers at the vaccination room, e.g. deploying staff from another cluster of Hospital Authority at the registration counter. Second, opinion differed on the ethical issues of vaccination – whether it is a duty to patients for nursing professionals. A local study found correlation between perceived moral responsibility and SIV uptake in nurses.27 It might be worthwhile to generate discussion and reflection among nurses on how vaccination, as a means of protecting patients and themselves, fit into the nursing professionalism in which they take pride. Third, the vaccinated nurses are mainly motivated by their own positive vaccination experience. But the question is how to make those nurses who have not yet had personal positive experience to get vaccinated for the first time. A study revealed that among HCPs, recommendations from colleagues, not from government or family members, was a cue to vaccination.28 Therefore, instead of having a few senior staff members as icons, it might be helpful to deploy many vaccinated nurses as ambassadors to influence their peers.  There are strength and limitations in this study. This is the first qualitative study on attitudes of primary care nurses on SIV in Hong Kong. Findings will inform future SIV campaigns to improve uptake amongst nurses. Regarding limitation of this study, the sample size is very small. Participants were recruited from only one cluster, with an overwhelming majority being female (only one male), and most being registered nurses. This sample profile limits generalisability of findings to all nurses in primary care in Hong Kong. There might be differences in viewpoint in different gender and ranks. For example, advanced practice nurses have more managerial role while the main role of enrolled nurses is providing clinical service. The interviewer and the interviewed nurses worked at the same cluster might lead to social desirability bias. Further study with larger samples is warranted. The COVID-19 pandemic has heightened the importance of SIV among healthcare workers. There are comments that in view of the uncertainty on the development of COVID-19 and its vaccine availability, increasing influenza vaccine upt ake by HCP is imperative in order to protect the essential healthcare services from influenza-associated absenteeism and the vulnerable patients they care for.29 A study found that the COVID-19 pandemic increased parents’ willingness to vaccinate their children against influence.30 Therefore, it is worthwhile to explore how the COVID-19 pandemic changes healthcare professionals’ attitude on personal vulnerability to infectious disease and effectiveness of vaccination as a preventive measure.
ConclusionThere are differences in attitudes towards SIV between unvaccinated and vaccinated nurses in primary care clinics. Strong belief on effectiveness of vaccination, based on personal experience, motivates vaccination. Lower risk appraisal, uncertainty in vaccine benefits, belief on alternative preventive measures were major barriers on SIV uptake in primary care nurses. Further direction of repackaging the SIV campaign might focus on respecting personal data privacy and autonomy, emphasising patient protection and a peer culture of vaccination.
AcknowledgementsThe authors thank all the nurses who participated in this research. The author gratefully acknowledge Mr. Clifford Kai-chung Wong for transcription of audio clips into transcripts, Dr. Yin-hang Chan for assistance in organising training in qualitative research, and Dr. Simon Sai-yu Lui for comment on the manuscript.Disclosure of potential conflict of interest This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. All authors declare no conflict of interest.
References
|
|