
|
March 2022,Volume 44, No.1
|
Update Article
|
Prostate cancer – screening, accurate diagnosis, and latest treatment strategiesFrancis CH Wong 黃俊謙,Peter KF Chiu 趙家鋒 HK Pract 2022;44:12-20 SummaryThe incidence of Pros tate cancer i s rapidl y increasing in Asia. While some prostate cancers are indolent and slow growing, the majority of prostate cancers being diagnosed still require treatment to avoid progression. Screening for prostate cancer can reduce metastatic disease and cancer mortality, but inappropriate screening can lead to over-diagnosis and over-treatment. Eligible men should undergo blood testing with prostate-specific antigen (PSA) as the first screening test. If PSA is found to be elevated, additional second tests including prostate health index (PHI), urine spermine and/or multiparametric MRI prostate can aid in selecting men that requires a prostate biopsy. MRI-guided targeted biopsy is recommended by guidelines to improve detection of significant prostate cancer. While radical prostatectomy and radiotherapy are recommended first line treatment of prostate cancer, novel focal therapies including highintensity focused ultrasound (HIFU) and Cryotherapy are valid alternatives with less complications in selected patients with focal tumors. In men with metastatic prostate cancer, androgen deprivation (hormonal) therapy should be combined with chemotherapy, radiotherapy or novel androgen receptor agents from the start to achieve the best survival outcomes. 摘要前列腺癌的發病率在亞洲正在迅速增加。雖然一些 早期前列腺癌生長緩慢,但大多數被診斷出的前列腺癌 仍需要治療以避免惡化。前列腺癌篩查可以降低轉移性 疾病和癌症死亡率,但不適當的篩查卻會導致過度診斷 和過度治療。適合篩查的男性應接受前列腺特異性抗原 (PSA) 血液檢測作為第一線檢測。如果發現 PSA 高於正 常,可以使用前列腺健康指數血液檢測 (PHI)、尿精胺尿 液檢測 (spermine) 或前列腺磁共振掃描 (MRI) 以確定進行 前列腺活檢的必要性。磁共振引導的靶向前列腺活檢可 以提高前列腺癌的檢測準確性。雖然根治性前列腺切除 術和放療是前列腺癌的第一線治療,但一些新的治療方 法包括高強度聚焦超聲 (HIFU) 和冷凍療法等的局部治療 也是有效的療法,可以減少治療並發症。對於患有轉移 性前列腺癌的男性,從一開始就應該接受荷爾蒙療法加上化學療法 、放射療法或新型雄激素受體藥物,以實現最佳的治療效果。 Introduction and Natural History of Prostate CancerProstate cancer, a common problem for both patients and doctors?Prostate cancer is known to be a common, yet, slow growing cancer. In Hong Kong, prostate cancer is the 3rd commonest cancer, with 2532 new cases every year, with a crude incidence rate of 64.6.1 In 20 years’ time, the incidence will be doubled.2 From a systematic review of post-mortem studies, for population older than 80 years old, around 50-60% was found to harbour indolent prostate cancer in autopsy.3 With the longer life expectancy nowadays, prostate cancer will be an increasingly common problem for both patients and doctors. Prostate cancer is mostly indolent and slow-growing, but some patients do die from itTraditionally, prostate cancer is known to be indolent most of the time. In elderly patients with prostate cancer, it is known that the majority of patients would not die from it. A landmark paper by Rider with the final update of 30 years follow up was published in 2013.4,5 223 Swedish men with clinically localised prostate cancer was treated with watchful waiting, and were subsequently treated with androgen deprivation therapy when there is symptomatic progression or metastasis. This study was well conducted with more than 30 years of follow up; 99% of patients died and reached the study endpoint for the final analysis. In the end, 64% patients did not require any androgen deprivation therapy and none of which has metastasis or cancer-specific mortality. Local progression was seen in around 40% of patients. Metastasis and cancerspecific mortality was seen in less than 20% of patients. Particularly, for men older than 75 years old, the cancer-specific mortality was 10% only. However, not all patients with prostate cancers can be safely neglected. From the Scandinavian Prostate Cancer Group Study Number 4 (SPCG-4) trial which studied around 700 patients in the pre- PSA era, prostatectomy is shown to reduce metastasis, improve cancer-specific and overall survival.6 From the Prostate cancer Intervention Vs Observation Trial (PIVOT), which studied more than 700 patients in the PSA era, prostatectomy is shown to improve cancer-specific mortality in a subset of patients with intermediate-risk localised disease.7 From the Hong Kong Cancer Registry, the proportion of prostate cancer that is diagnosed at an advanced stage is high (27.9% diagnosed at stage 3; and 26,1% diagnosed at stage 4 (i.e. beyond localised disease with N+ or M+ diseases)), and prostate cancer is still the 4th commonest cause of death in Hong Kong.8 Therefore, the key is to diagnose and treat clinically significant and potentially aggressive cancer at an earlier stage, while not over-diagnosing and over-treating some indolent ones. Screening: Why? Who? How?Screening: why screening?Whether prostate cancer screening is beneficial to the community has been a topic of hot debate. With reference to the WHO criteria by Wilson and Jungner, prostate cancer screening probably can fulfil some of the criteria in being an important health problem, with a readily available diagnostic test and standard treatments, with a recognisable latent or early symptomatic stage, and an adequately understood natural history. However, traditionally, there were some concerns regarding whether the diagnostic test (i.e. transrectal prostate biopsy) is safe, whether there is an agreed policy of whom to treat, whether the earlier treatment carries survival benefits without compromising on the patient’s quality of life, and whether the cost of case finding is economically balanced. With recent developments and publications of multiple high quality trials, the traditional concerns of prostate cancer screening can be lessened and reassured. The details concerning the diagnostic tests and treatment developments, which further favours prostate cancer screening, will be further discussed in the following sections. For prostate cancer screening, the current best evidence comes from the ERSPC trial (European Randomised Study of Screening of Prostate Cancer).9-11 In this trial, 182,000 men, aged 55-69 years old, in 7 European countries were randomised into the screening group with PSA once every 4 years with prostate biopsy when PSA >3.0, and the control group with no PSA testing. The trial was published in 2009, 2014 and 2019 with the latest update after 16 years of follow-up data. PSA screening for prostate cancer has been showed to be beneficial in preventing prostate cancer deaths, with a relative risk reduction in cancerspecific mortality of 21%. To prevent one prostate cancer death, the number needed to screen (NNS) is 570 and number needed to treat (NNT) is 18. The benefit of prostate cancer screening is shown to be comparable to that of breast cancer screening with a NNS of 570 as well. Screening: who to screen?The decision on whom to screen should take into consideration several factors. The most important risk factors for prostate cancers are age, ethnicity, and family history. With regards to a patient’s age and comorbidities, the younger or fitter the person is, the greater the potential benefit for prostate cancer screening is. Life expectancy of Hong Kong men has surpassed 80 years old, one of the longest in the world.12 Given the long life expectancy, even early localised prostate cancer can progress within this long lifespan, and so early screening, detection and treatment of prostate cancer should be considered. There recommendation from Hong Kong Urological Association in 2013 was13:
The recommendation from the American Urological Association in 2018 was14,15:
For ethnicity, it is known that African-Americans and Caucasians have a higher incidence of prostate cancer when compared with Asians. In a local study by The Chinese University of Hong Kong, for Asian patients with PSA 4-10, prostate cancer diagnosed on biopsy was only approximately 50% of that in Caucasian men.16,17 For those with a family history of prostate cancer, the relative risk increases for one, two and three firstdegree firstdegree relatives are approximately 2-folds, 5-folds and 11-folds respectively.18 A Nordic twins study showed that the inheritable component of prostate cancers was up to 42%.19 Therefore, for patients with a strong family history of prostate cancer, more aggressive screening is worthwhile.
Screening: What is PSA?PSA has revolutionised prostate cancer screening since early 1990s. Prostate specific antigen (PSA) is a glycoprotein that is secreted by prostate ductal epithelial cells. Hence, it is an organ-specific marker but not a disease-specific marker. An elevated PSA can be due to conditions including prostate cancer, benign prostatic hyperplasia, urinary tract infection, prostatitis, urinary retention, recent ejaculation, recent transurethral instrumentations or digital rectal examination, etc. PSA has a half-life of 2.5-3 days. Therefore, in patients with an elevated PSA, but with a possibly “falsely” elevated PSA due to other conditions such as recent urinary tract infection, a repeat PSA testing at approximately 4 weeks interval is a reasonable way to delineate.
Screening: PSA, what is normal and how does PSA predict prostate cancer?PSA normal range is commonly defined as <4.0. This cut-off value is based on the landmark paper by Catalona et al back in 1990s.20 The possibility of prostate cancer in Caucasians with a PSA <4, 4-10, >10 were 11%, ~25% and ~65% respectively.17 In Hong Kong, with the majority of the population being Chinese in ethnicity, the chances of developing prostate cancer for the various PSA levels were henceforth noted to be lower than that for Caucasian men with the same level. This is shown in Table 1 from data published by the CUHK.16
Screening: Apart from PSA, other risk-stratification tools are availableProstate Health IndexProstate health index (PHI) is a commonly used risk-stratification tool adopted by urologists in Hong Kong since 2016. Prostate health index is calculated with a formula incorporating p2PSA, PSA (both higher in prostate cancer patients) and free-PSA (lower in prostate cancer patients).21 Validation study on PHI use in Hong Kong Chinese has been published by the CUHK.22 Ethnic and region-specific reference range is also available.23 With the available data, better patient counselling can be done before deciding on prostate biopsy. Apart from PHI, 4K score is another blood test based risk stratification tool but is only available in selected regions in North America and Europe.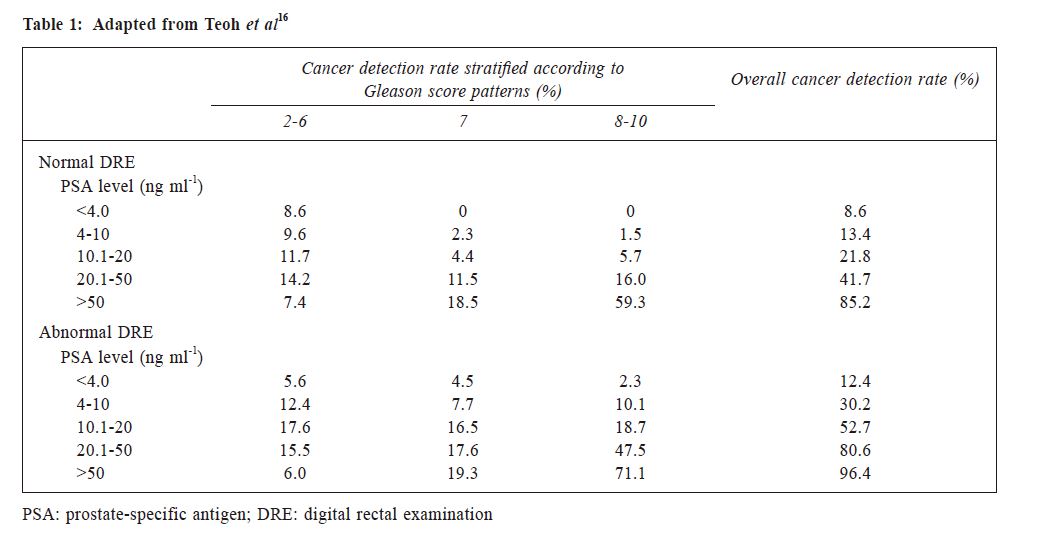 Urine tests have also been used as risk-stratification tools. PCA3 test detects PCA3 gene, a non-coding segment of mRNA, which is produced more in prostate cancer cells.24 Urine PCA3 has been commercially used in North America and Europe since 2013, but its performance has been shown in some series to be inferior to the PHI blood test.25 Another test called SelectMDx measures the expression of two mRNA cancer-related biomarkers (HOXC6 and DLX1) in urine, and in combination with clinical factors, stratifying men into higher and lower risks of significant prostate cancer.26 However, both urine PCA3 test and SelectMDx test requires an attentive prostatic massage (6 strokes on the prostate gland) immediately before urine sampling, which increases the patient’s discomfort and inconvenience at specimen collection. Furthermore, the use of these urine tests has been limited in Asia due to high cost and the need for them to be sent to laboratories in Europe or America for processing. The Urine Spermine test is a newly developed simple urine test which does not require an attentive prostatic massage before urine collection. It was developed in Hong Kong with Chinese men as subjects. The Spermine level was found to be lower in prostate cancer tissues and lower in urine of men with prostate cancer. A large local study has shown that the Urine Spermine test is able to predict the risk of significant prostate cancers.27 Also, by combining other parameters such as age, digital rectal examination, PSA, prostate volume, the Urine Spermine risk score was developed and this further improved the prediction of the presence of significant prostate cancers.28 Using a Spermine risk score cutoff of 7, the test achieved a sensitivity of 90% and negative predictive value of 95.4%, while reducing 36.7% unnecessary prostate biopsies. 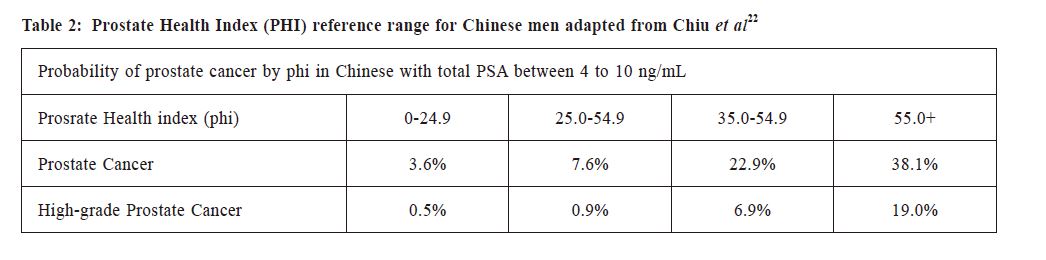 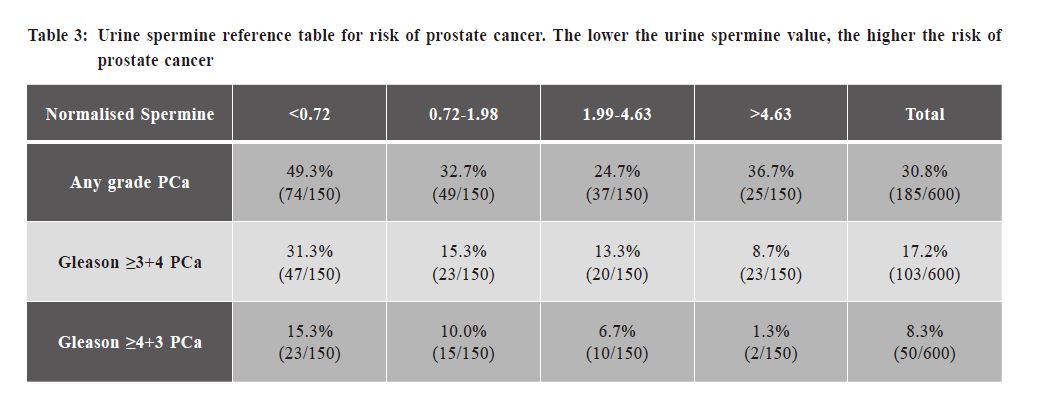
Diagnosis: major changes have undergone recent yearsDiagnosis: How is prostate biopsy done nowadays?For patients with a clinical suspicion of prostate cancer e.g., elevated PSA, abnormal digital rectal examination of prostate or family history of prostate cancer, diagnosis of prostate cancer traditionally would involve a transrectal 12-core systematic biopsy (TRUS biopsy). TRUS biopsy is a local anaesthetic procedure, done with the patient lying laterally with hips and knees flexed, with multiple prostate biopsies taken through the rectum under the guidance of a transrectal ultrasound probe. However, TRUS biopsy carries risks and morbidities, particularly the risk of severe sepsis (3-5%) and per-rectal bleeding (~2%) requiring hospitalisation and treatments.29Since 2018-2019, transperineal prostate biopsy has gradually replaced transrectal prostate biopsy as the biopsy route of choice in Hong Kong. With the transperineal route, needle puncture is now through sterilised perineal skin rather than through the rectum with faecal bacteria flora. The most concerning procedural complication of post-biopsy sepsis is reduced from up to 6.3% in transrectal biopsy down to nearly 0% in transperineal biopsy.29-31 The risk of perrectal bleeding is also avoided. Other complications including urinary retention (1-5% risk)30-32, post-biopsy haematuria31 were similar to TRUS biopsy. Also, the transperineal prostate biopsy is proven feasible under local anaesthesia and can be performed as a day case under an office setting.31,33 Overall, the safety of prostate biopsy has greatly improved in recent years. Diagnosis: is prostate biopsy accurate?Magnetic resonance imaging(MRI ) of the prostate is increasingly adopted by urologists in the diagnostic pathway for prostate cancer, and has been recently incorporated into the international guidelines since 2019.34 Multiparametric MRI prostate involves difference phases of MRI (T2W, DWI, ADC and DCE phases). If MRI contrast usage is contraindicated for the patient, a non-contrast MRI scan (biparametric MRI with T2W and DWI phases) can provide comparable diagnostic accuracy while saving up to 30-40% scanning time.35 Interpretation of the MRI has been guided by a validated scoring system, the Prostate Imaging Reporting And Data System (PI-RADS) version 2.1.36 The results of MRI prostate will be reported under the PI-RADS scoring system from 1 to 5. The probability of harbouring a clinically significant prostate cancer (i.e., Prostate cancer grading Gleason score of 7 or above, out of 10) is approximately 20%, 60%, and 80% for PIRADS 3, 4, and 5 respectively.37,38 MRI alone is not diagnostic of prostate cancer, and MRI cannot substitute the need for prostate biopsy in the confirmation of prostate cancer. If MRI shows suspicious lesions (i.e. PI-RADS 3 or above), the urologist can add targeted biopsies to the suspicious lesions on top of systematic biopsies, which have been shown to improve the cancer detection rate for clinically significant prostate cancer by an additional 10%.37,39,40 Various techniques are available to allow the urologist to accurately target the lesion for biopsy. Commonly used technique would be MRI/TRUS fusion biopsy with dedicated software and hardware to fuse the MRI films with the realtime ultrasound imaging for targeting. Other targeting techniques include cognitive fusion and MRI in-bore biopsy have comparable accuracy in expert hands.41 However, cognitive fusion may not be reliably accurate in the hands of the average Urologists, especially if the scenario is that of a small lesion in a relatively larger prostate. The equipment required for MRI in-bore biopsy is not readily available in Hong Kong and in most hospitals in the world, and therefore this technique is rarely used. If the MRI shows no suspicious lesions (i.e., PIRADS 1 or 2), the chance of a clinically significant prostate cancer would be only 11%.37 Hence, the patient might be counselled on the alternative option of PSA and/or MRI monitoring rather than invasive prostate biopsy. Therefore, adding MRI nowadays allows better risk-stratification and better patient counselling before prostate biopsy. It also enables targeted biopsy and improves the diagnostic accuracy in detecting clinically significant prostate cancers.38-40 Diagnosis: StagingFDG PET scan is well known to be insensitive in detecting metastasis for advanced prostate cancer. Discovery of the radioligand PSMA (Prostate-Specific Membrane Antigen) has revolutionised the diagnostic imaging for metastatic or recurrent disease. PSMA PETCT scan was shown to be superior to conventional imaging (bone scan plus contrast CT) by 27%.42 Furthermore, theranostic (ability to use an organ specific ligand and label it to both a diagnostic/imaging and therapeutic agent) with PSMA can be used to treat metastatic disease in selected patients, by combining therapeutic Lutetium-177 to PSMA ligand.43
Treatment: Risk-stratified evidence-based treatment approach is increasingly being adopted, alongside with the promising evolution in new treatment optionsTreatment: an agreed policy to whom to treat?Given the indolent course of prostate cancer in the majority of cases, whether to keep the patient on surveillance or active treatment has been a topic of discussion. In recent years, several publications have shed light on guiding our decision-making.Localised prostate cancers can be stratified into low, intermediate and high risk according to the PSA level, Gleason Score and clinical T-staging.44-46 For low-risk localised disease, the PROTECT trial has shown that in 10 years time, only about half of the patients randomised to Active Monitoring required treatment, and the oncological outcome in terms of cancer-specific survival is the same with Active Monitoring, Radical Prostatectomy, or Radical Radiotherapy.47 Therefore, it is strongly advocated not to over-treat low risk localised prostate cancer. For intermediate-risk and high-risk localised disease, the chances of disease progression and cancerspecific mortality increases.48 Hence, active treatment is usually advised. 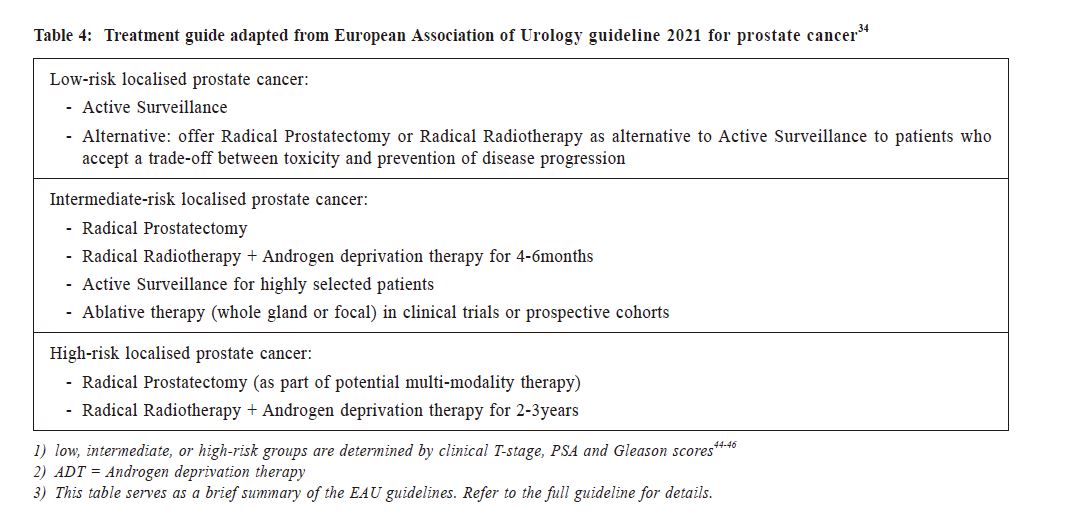
Treatment: prostate cancer treatments carry significant complications and will significantly worsen the quality of life?Treatment of localised prostate cancer traditionally would be surgery with radical prostatectomy or radiotherapy with radical radiotherapy, which both carries significant comorbidities.For radical prostatectomy, the urologist has progress from open, to laparoscopic and now to roboticassisted minimal invasive surgeries. With robotic radical prostatectomy, the operative time, intra-operative blood loss and post-operative recovery and early functional recovery (continence) have been significantly improved.49, 50 Moreover, robotic surgery enables finer dissections, higher degree of freedom, and significantly shorter learning curve.51-53 Almost all radical radiotherapies for prostate cancer are in the form of external beam radiotherapy (EBRT) in Hong Kong. Image-guided RT (IGRT) and Intensitymodulated RT (IMRT) has significantly improved the accuracy of prostate irradiation and reduced irradiation injury to surrounding organs like rectum and bladder. Fiducial markers and hydrogel rectal spacers are further tools to reduce radiotherapy toxicities.54,55 Traditionally, patient is required to visit the hospital for more than 30 times for multiple fractions of hyperfractionated radiotherapy. Nowadays, with stereotactic body radiotherapy (SBRT), a hypofractionated radiotherapy approach can reduce number of RT sessions to about 5-10. This reduces the number of fractions and hospital visits required with similar oncological control and toxicity profile.56 For those prostate cancers limited to a focal part of the prostate that can be visualised on MRI imaging, focal therapy with various energies is an alternative. The most commonly used focal therapies worldwide are high intensity focused ultrasound (HIFU) and cryotherapy.57,58 Other options like Irreversible Electroporation (IRE), Targeted Microwave Ablation (TMA), Photodynamic Therapy (PDT), and laser ablations are promising alternatives under development. The advantages of focal therapies include minimal treatment morbidity, almost zero incontinence, preservation of sexual function, and avoidance of irradiation injury. Although focal therapy has a higher recurrence rate compared with radical surgery or radiotherapy, repeated focal treatment or salvage radical treatment are both feasible options.57 HIFU, cryotherapy, and targeted microwave ablation (TMA) has been performed in selected hospitals in Hong Kong in the past few years. For androgen-deprivation therapy, operation with bilateral orchidectomy is traditionally required. Nowadays, androgen-deprivation therapy can be achieved by regular LHRH (luteinising hormonereleasing hormone) agonist or antagonist injections. Recently, an oral LHRH antagonist was developed and currently available in North America.59 It is expected to be available in Hong Kong within 1-2 years’ time.
Treatment of locally advanced, oligometastatic, and metastatic prostate cancersFor locally advanced disease, curative intent treatment can be offered with radical radiotherapy with 2-3 years of androgen deprivation therapy. Radical prostatectomy can also be offered as part of multimodality therapy. For patients unable to receive local treatments, immediate androgen deprivation therapy has been shown to be of benefit in the subsets of patients with aggressive disease (i.e. PSA doubling-time <12months, PSA >50ng/ml, poorly-differentiated tumour or troublesome local disease-related symptoms).60For metastatic disease, traditional treatment would be ADT alone. However, studies have shown that adding early upfront chemotherapy or newer hormonal agents carry an overall survival benefit.61-64 For oligometastatic disease (i.e., low-volume metastatic disease), adding radiotherapy to the pelvis also carries an overall survival benefit.65 Therefore, even for advanced disease, earlier detection of prostate cancer allows earlier treatment with additional survival benefits.
Treatment of castration-resistant prostate cancers: multiple new therapies availableTreatment of IDAThe majority of prostate cancers respond well to androgen deprivation therapy initially. However, with time, castration-resistance develops with a mean duration of 14 months. Currently, various treatment options are available: Chemotherapy including docetaxel and cabazitaxel66-68; Novel hormonal agents including abiraterone, enzalutamide, etc.69-75; Interventional nuclear medicine therapies including Radium-22376, Lutetium-177–PSMA-61743; Immunotherapy includings Sipuleucel-T77; and last but not least, targeted therapy with PARP inhibitors like Olaparib for men with specific genetic mutations.78 With the exception of Sipuleucel-T, all of the above new therapies for castration resistant prostate cancers are available in Hong Kong.
ConclusionWith the advancements in prostate cancer diagnosis and treatment strategies, the traditional concerns of over-investigation, over-diagnosis and over-treatment with prostate cancer screening have significantly reduced. An optimised prostate cancer screening pathway could accurately diagnose men with clinically significant prostate cancer and allow early precision treatment. This would hopefully aid to achieve our ultimate goal in minimising metastatic disease and prostate cancer mortality in Hong Kong.
Francis CH Wong, MBBS, FRCSEd(Urol), FHKAM(Surg)
Correspondence to: Dr Peter KF Chiu, Department of Surgery, 4/F, LCW Clinical Sciences Building,
Prince of Wales Hospital, Shatin, N.T., Kwun Tong, Kowloon,
Hong Kong SAR.
References:
|
|