
|
September 2022,Volume 44, No.3
|
Caes Report
|
Interpersonal psychotherapy for complicated grief - an introduction for family physiciansKimberly KY Yip 葉健欣,Joseph PY Chung 鍾沛然 HK Pract 2022;44:69-75 SummaryComplicated grief is a condition that is commonly encountered in the primary care setting. It is often overlooked, yet it can cause significant impairments in those who are grieving. Family physicians are often the first medical professional to come across bereaving patients, and some of these patients may be suffering from complicated grieving. Family physicians can refer them for appropriate treatment. Interpersonal psychotherapy (IPT) is one evidencebased psychological treatment of complicated grief. It is a time-limited therapy to facilitate the griever to mourn for the loss, and rebuild social support through improving communication and interpersonal effectiveness. This report is an educational article with an aim to give family physicians a glimpse of one evidence-based psychological treatments of complicated grief. Keywords: Interpersonal psychotherapy, IPT, complicated grief, pathological grief, grief, bereavement
摘要複雜的哀痛在家庭醫學逐漸普及。悲傷反應是失去至 親的一個自然的情緒反應。若不處理好,便會演變成複雜 哀痛,對生活造成嚴重的影響。家庭醫生是病人最先尋求 協助的醫護人員,也最先能夠給予經歷悲傷反應的病人治 療。人際心理治療(悲傷反應)是其中一種被臨床研究證 實對複雜哀痛的有效治療。人際心理治療是一種方便和容 易進行的心理治療。人際心理治療是一種限時、可操作性 的治療。通過適當的人際關係調整,分析,病人可以學會 把情緒和人際關係聯繫起來,改善溝通和其他人際關係, 係來減輕抑鬱。作者希望透過這報告,說明人際心理治療 的原則和技巧,令人際心理治療在家庭醫學普及化。IntroductionGrief is a psychological and behavioural response to bereavement, or any kind of loss.1 It has highly variable presentations across different cultural groups. It is an almost inevitable experience for most people, and is commonly encountered in the primary care setting. Different modelsVarious models have been used to describe the clinical features and course of grief. Most of these models are based on the stage theory of grief, dividing it into different stages with specific emotional and behavioural responses. One of the first theories developed was the four phases of grief by Bowlby2 and Parkes3, based on Bowlby’s attachment theory. The four phases are (i) shock and numbness, (ii) yearning and searching, (iii) disorganisation and despair, and (iv) reorganisation and recovery. Another well referred to model would be the Kubler-Ross model4 originally used to describe the grief faced by patients with terminal illnesses. The stages include (i) denial, (ii) anger, (iii) bargaining, (iv) depression, and (v) acceptance. The duration of grief again varies greatly, usually from 6 to 12 months. In Maciejewski and colleagues’ study5 of 233 individuals who were grieving deaths caused by natural causes, the authors found the indicators of their grief, (i) disbelief, (ii) yearning, (iii) anger, (iv) depression, ending with (v) acceptance, all peaked within 6 months. Complicated grief is characterised by a prolonged and abnormally intense grief reaction, with a prevalence of 6.7% after major bereavement.6 Though there are no definite diagnostic criteria for complicated grief, ICD-11 describes one condition ‘Prolonged Grief Disorder' that illustrates the features of complicated grief.7 To meet the diagnostic criteria, one needs to experience persistent and pervasive longing for the deceased, and/or preoccupation with the deceased, combined with 10 additional grief reactions for at least 6 months after bereavement. Similarly, DSM V has also considered persistent complex bereavement disorder as a condition for further study. Persistent complex bereavement8 disorder also includes key features of persistent yearning and longing for the deceased, and preoccupation with the deceased in their diagnostic criteria. The only major difference would be the duration of the disorder being at least 12 months for DSM V, compared to only 6 months in Prolonged Grief Disorder. Treatment for complicated grief should be given promptly as it affects the person’s quality of life9, and has impact on both psychiatric and physical well-being. 55% of those suffering from complicated grief together with comorbid depression.10 It is also associated with increased cardiovascular accidents and elevated cancer risks.11 Therefore, psychological treatment to grievers and early identification of complicated grief in the primary care setting are important in order to improve quality of life and to prevent further complications. Current treatment for complicated grief include both pharmacological treatment with antidepressants, and any one of the psychological treatments such as the complicated-grief therapy, cognitive-behavioural therapy and interpersonal psychotherapy. The choice of psychotherapy depends on the availability of local expertise. Whereas complicatedgrief therapy and cognitive-behavioural therapy require more training, IPT techniques are easier to learn. The goal of IPT in grief patients is to facilitate mourning and to increase social support, thus reducing depressive symptoms. The effectiveness of IPT has been shown in randomised controlled trials.12 The case below illustrates the use of IPT in the treatment of complicated grief. The clinical and personal details have been changed so that not to identify the patient. The casePresenting problemMr. W was a 70-year-old retired driver and was living with a 20-years old son. He was referred to us because he had been having 12 months’ of persistent low mood precipitated by the death of his wife. His persistent depressive mood had limited response to antidepressant treatment. His wife had committed suicide by jumping off from a height at home. He presented with a pervasive low mood and crying spells, initial insomnia, and loss of interest. He felt guilty for not being able to prevent his wife’s death. He blamed himself for not being able to provide her with a better life. He became withdrawn and stayed at home all the time. His appetite was, however, maintained. He did not have any suicidal ideation, as he felt a responsibility to take care of his son. He would keep the couple’s bed room the same and change the bed sheets for his wife regularly. Every day, he would make visits to the pier where the couple had their first few dates. However, he had not reported any psychotic symptoms. He was diagnosed with complicated grief and mild depressive episodes. He was prescribed with Mirtazapine 30mg every night, with little improvement in sleep. His mood remained low all the time. Previous psychiatric history:Mr. W had previous psychiatric history before. He was diagnosed with Adjustment Disorder with depressive features when he first presented to a psychiatric clinic 10 years earlier. He suspected his wife was having an extra-marital affair which precipitated his low mood. No medication was prescribed throughout. He was only given some hypnotics to improve his sleep and his mood and sleep improved somewhat after a few months along as the couple’s relationship improved. There had been no violence or self-harm history. Mr. W had received regular follow up at the psychiatric outpatient clinic since then till present day.
HistoryMr. W’s family does not have any serious past history of medical or mental illness. Mr. W has diabetes mellitus with complications of diabetic nephropathy and diabetic foot ulcers. He also suffers from hypertension.Mr. W is locally born and raised. He received three years of formal education. He had one elder sister and three younger brothers. His mother, a housewife, left home when he was 5 years old due to marital discord. His mother later re-joined the family when Mr. W was in his teenage years for reason that was not known to him. He had idolised his mother, whose words he considered to be very wise and were still remembered very clearly till this day. His father was a barber who remained distant to Mr. W most of the time. During his teenage years, he was often made fun of by his classmates and colleagues, for being ‘dim’. His mother and his siblings had also told him that he was the “dimmest” in the family. Mr. W worked as a private driver for almost thirty years. He married his wife when he was 50 years old. The couple met through a friend when Mr. W was visiting mainland China. His wife was 20 years younger. While Mr. W was still in China, he offered to marry his wife initially mainly to help her gain Hong Kong citizenship. The couple later fell in love and had a son together. The wife and son came to Hong Kong from China 2 years later. After the wife came to Hong Kong, she was diagnosed with depression and had been prescribed antidepressants.
Personality traits, cultural and religious factorsMr. W had low self-esteem as he perceived himself to be stupid. He had difficulty trusting others due to a fear of being taken advantage of – that was because that his mother had frequently told him. He described himself to be a family-oriented and responsible person. He valued the “family” a lot but never considered marriage as he felt he was not capable of providing another person or children with a good life. He was introverted and had few friends as his mother warned him that others could easily betray him. He himself avoided having too many friends or had little interaction with others as a result of his low self-esteem. He did not want to ‘bother’ others so he did not reach out to anyone, including his siblings, which perpetuated his social isolation.Mr. W believed that a loyal partner, and an unbroken family as being very important in the Chinese culture, as it signified a man’s success in fulfilling his role to form, and maintain a “complete” family. He also believed that it is solely the role of the man of the family to provide for the family. Mr. W had no religious beliefs.
Diagnosis and managementClinical assessmentClinical assessment was performed in the first few sessions. An introduction to the structure, goals and nature of Interpersonal Psychotherapy was given. This was followed by history taking to establish a diagnosis. The interpersonal inventory and interpersonal formulation would then follow, assessing the social network and attachment style, as well as to identify an area of focus. Goals of the therapy would be set collaboratively with the patient.
Session 1In the first session, a psychiatric history was taken for further clarification of Mr. W’s depressive and grief symptoms. The principles and aims of IPT, along with Mr. W’s expectations were discussed.
Session 2 - 4In sessions 2 and 3, Mr. W’s attachment style and interpersonal pattern were explored. To identify his attachment style, specific questions were asked about his relationship with his parents. For example: “Tell me about the way you were brought up”. “How did your parents relate to you”? “what was your relationship like with your siblings”? “Tell me about your relationship with your peers”.It became clear after discussion with Mr. W that his view on himself and others showed an avoidant attachment style. . This was contributed by the lack of a maternal figure at a young age when his mother left the home, and how he had been told since young that he was stupid, thus resulted in him avoiding contact or establishing any relationships with others. His insecurity was also evident when he had been in a relationship prior to getting married as he was afraid of being deserted by his partner. During the third session, Mr. W was asked to fill in the interpersonal inventory: a diagram of 3 concentric circles, representing his interpersonal network ( Figure 1 ). We asked Mr. W to write down 6 - 7 names; the closest ones in the most inner circle, while the not so close ones at the outermost circle. We reminded Mr. W that names of deceased persons should not be written down, as IPT focuses on here and now, and only his current social network should be assessed. We then asked Mr. W to describe the relationship with each of these important people. It is important to ask patients to write down the names on their own, as this would allows patients to open up to the therapist, to reflect on their own relationship with significant others, and to help the therapist identify any interpersonal patterns. 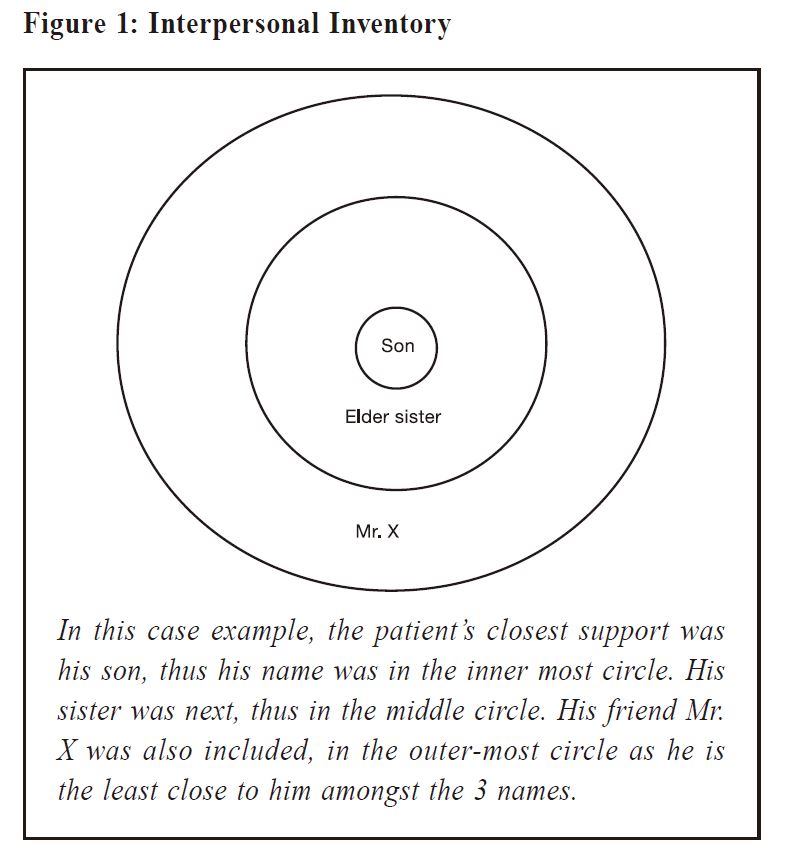
In Mr. W’s case, he had very limited social support. He put the name of his son in the innermost circle. He was only able to put down the name of his elder sister after much prompting in the middle circle. No further names were written down. We have found the establishment of an interpersonal circle to be a very useful tool in the primary care setting, for patients to open up to talk about their relationships. In the fourth session, the interpersonal formulation was completed. The interpersonal formulation is based on a bio-psychosocial, cultural and spiritual model, as suggested by S Stuart. (Figure 2) Guided by the therapist, the patient was asked to fill in factors under each category that could have contributed to his distress. It is again important for the patient to fill this in on his, or her own, after being guided by the healthcare provider, as it allows them to appreciate the many factors contributing to their current presentation, gaining an insight into their problem. Referring back to Mr. W, psychologically, he had always felt inadequate and inferior. His low selfesteem had contributed to his depression. His perceived inferiority had also perpetuated the self-blame that he had for not being the “perfect, smart, interesting husband”, and the idea that his deceased wife should have a “deserved better” deal. This had also prevented him from reaching out to his friends and siblings, as he did not want to “bother” others. He perceived himself as “boring”, thus avoided contact with others. Cultural factors would include his value of a “complete family”. The loss of his wife had his family “broken” which he found very difficult to accept, thus leading to his depression and complicated grief. Treatment goals were set by the end of the session 4 with Mr. W, aiming to reduce his depressive symptoms, to build on his social support, and to enhance communication with his son. 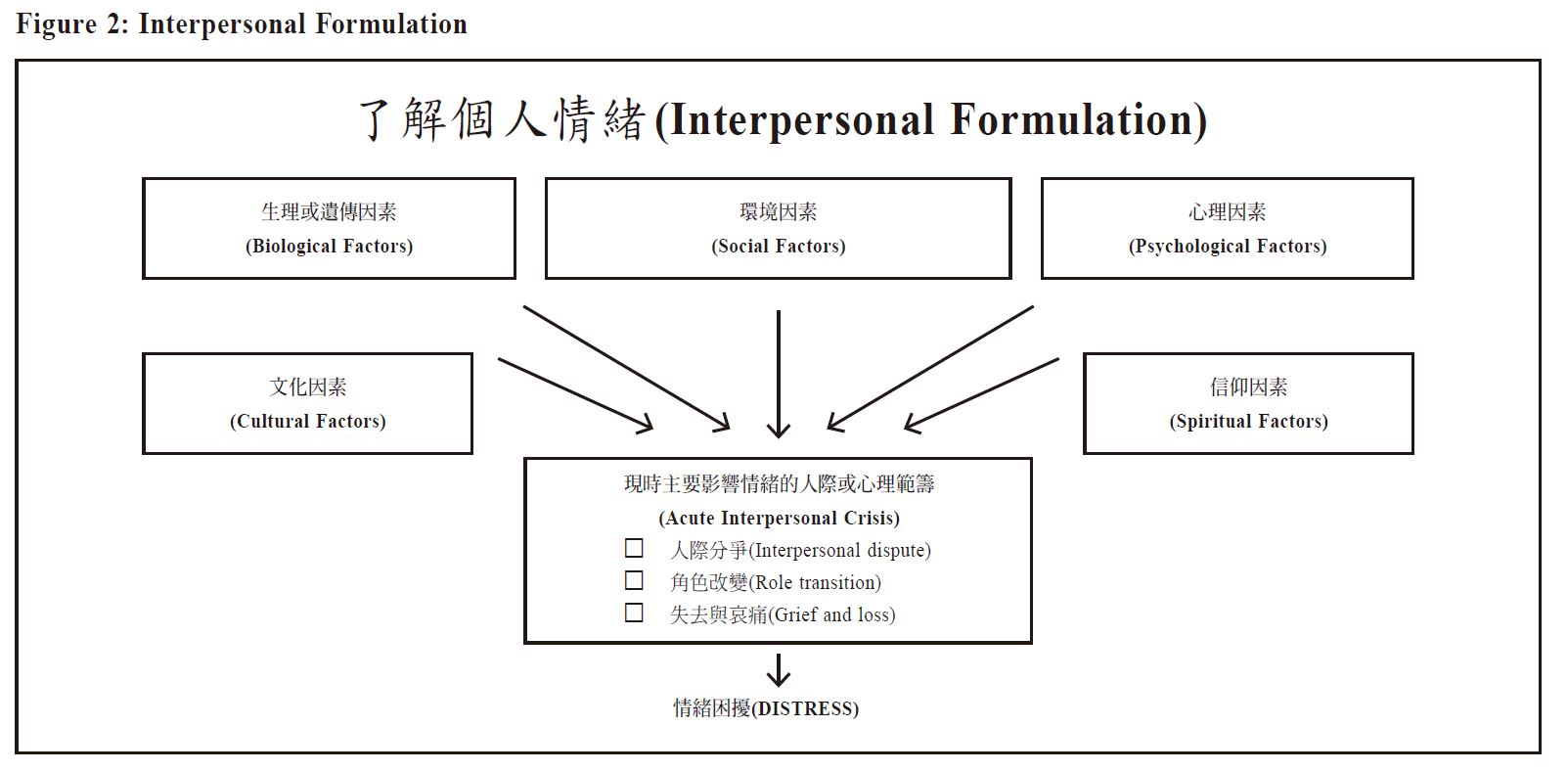
The middle work phaseThe two specific tasks in the work phase for complicated grief are to: first facilitate mourning; and second, to improve the patientʼs social support.Common techniques used in this phase includes clarification and reconstruction of the relationship with the deceased, communication analysis, facilitating and encouraging expression emotions, and role-playing.
Session 5 - 6In sessions 5 and 6, the therapist asked Mr. W to describe in detail his relationship with his wife, and how it had evolved through their married years. Details of how the couple met, how their relationship had developed into marriage, the good and bad days in the relationship were asked. The deceased wife was often idealised, therefore both the good and bad about her relationship to him was asked, in order to make a 3-dimensional reconstruction. It was revealed that the couple’s relationship turned distant after his wife was diagnosed with Depression. The therapist reminded Mr. W of the biological model of depression and how it had led to his wife’s low mood, irritability and possibly subsequent suicide, in order to relieve the patient’s guilt and sense of responsibility towards her death.Mr. W’s commitment and efforts put into the marriage were acknowledged and validated in these sessions, to remind him, and to relieve his self-blame of not doing ‘enough’. The therapist also encouraged and assisted Mr. W to express, identify and to verbalise his emotions - which he found difficult to do, possibly due to his low educational level - as he described specific incidents of their relationship.
Session 7 - 10In subsequent sessions, Mr. W was asked to recall the details and events that took place: before, and around the time of the death of his wife. The aim of session 7, was to help him to organise, and reconstruct the experience as part of facilitating mourning. In session 8, the changes that took place after the death of the deceased were discussed. It is important to allow the client to talk about events around the time of the deceased’s death with its associated feelings. The therapist asked Mr. W: “What were you feeling at the time?” “How did you feel after receiving the news of your wife’s death?” to explore the suppressed emotions - which were described as “being in shock”, “numb”, “disbelief” and then later “immense sadness”, “feeling angry at myself”, “feeling angry at her for jumping off the building that easily”, to finally ‘“guilt”. It was through helping Mr. W to identify and express his emotions, that he was able to successfully mourn the loss of a loved one.In sessions 9 to 10, the focus was to build his social support, mainly by working on his relationship and communication with his son. Specific techniques such as brainstorming, communication analysis, and role-play were used. The relationship between his son was clarified again using specific interpersonal incidents to establish the pattern of communication between Mr. W and his son. Specific questions such as “what did you do when your son said that”, “What did you say to him?” were asked, as well as questions about Mr. W’s emotions: “How did that make you feel?” “What was going through your mind then?’ ‘What did you expect him to do, or say?’ The therapist brainstormed with Mr. W different ways to express his love towards, and to start conversations with his 20-year-old son. Communication analysis was performed to identify any ambiguous, indirect, or lack of communication with his son, for example, assuming that his son knows what was on his mind, thus never verbally expressing any of his thoughts or ideas to his son. His belief that traditional Chinese men did not have to be affectionate or expressive, contributed to the lack of communication with his son, and this was discussed during therapy. Role-play was then used to assist Mr. W to develop new perspectives on his communication style with his son, in order to understand his communication pattern. It is important here to have the patient play the significant other first as it helps them to see from another perspective.
Concluding sessionsIn the concluding sessions 11 and 12, the goals set at the beginning of therapy were revisited. Both patient and therapist agreed that there was significant improvement in Mr. W’s mood. His self-blame and guilt had resolved and he was less withdrawn and had regular contact with his siblings. He was also less worried about his son as the two had more communication compared to before, when they did not know what each other was thinking. His clinical improvement was supported by the improvement in his Patient Health Quetionnaire-9 (PHQ) score, from “18” in the first session, to a “2” at the end of the 12 sessions. His Hamilton Depression Rating Scale (HDRS) had also reduced from “19” in the first session to “2” in the last session.
DiscussionThe above case illustrated the principles and techniques of conducting IPT in patients with complicated grief. IPT helps patients to process their grief and help them adjust to a life after the loss of a loved one, by improving communication with family and friends and rebuilding their social network.The framework of IPT in complicated grief includes: (1) obtain a psychiatric history, conduct an interpersonal inventory and interpersonal formulation in the initial 2 - 3 sessions, (2) facilitate mourning and rebuild social support in the middle phase, and (3) review gains in treatment, manage separation anxiety and educate on symptoms of relapse in the concluding few sessions. Common IPT techniques in the middle phase includes clarification, facilitate expression of emotions, communication analysis, role play and decision analysis. Although conducting a 12-session psychological treatment in the primary care setting may be difficult, many of the techniques in IPT, include facilitating the expression of emotions, building social support, can easily be applied by the family physician in his/her routine clinical setting.
ConclusionFamily physicians are often the first medical professional to come across bereaving patients. We hope the above case demonstration can help family physicians gain a glimpse of a specific psychological treatment available for treatment of complicated grief. Further information about IPT and training information can be found on the website of the International Society of Interpersonal Psychotherapy.
References
|
|