
|
September 2022,Volume 44, No.3
|
Case Report
|
A case of sterile pyuria caused by urological tuberculosisEsther SC Pang 彭詩情 HK Pract 2022;44:78-80
SummaryFor a patient wi th diabetes , an albumin-to-creatinine ratio (ACR) test is ordered yearly to screen for proteinuria. We should not assume that the cause of new-onset proteinuria is always diabetic nephropathy. Curable causes like urinary tract infection should be ruled out if the patient is symptomatic. To confirm the diagnosis of urinary tract infection, a mid-stream urine culture is saved. Occasionally, we encounter sterile pyuria. The absence of bacteria from the routine urine culture does not always rule out infection. Atypical infection by Mycobacterium tuberculosis is an important cause of sterile pyuria.
摘要對於糖尿病患者,醫生每年都要查驗尿白蛋白肌酐 比值(ACR),以篩查蛋白尿。我們不應認為新發蛋白尿 的病因一定是糖尿病腎病。如果病人有症狀,應排除尿 路感染等可治癒的病因。為確診尿路感染,可保留中段 尿液進行培養。我們偶爾會碰到無菌性膿尿。常規尿液 培養中未見細菌並不總能排除感染。結核分枝桿菌的非 典型感染是導致無菌性膿尿的重要原因之一。
Case presentationA 62-years-old lady with diabetes and hyperlipidaemia had regular follow-ups at the general outpatient clinic. She was not on medication for both conditions. She was a non-smoker. Her latest Hba1c was 6.5%. In the annual screening test in November 2019, she was noted to have new-onset proteinuria, the urine albumin- to-creatinine result was 48 mg/ mmol (normal < 2.5mg/mmol). She revealed symptoms of frothy and cloudy urine for a few months, with frequency and urgency of urination. She did not have dysuria, haematuria, abdominal pain, or fever. Because of the presence of urinary symptoms, a mid- stream urine culture test was ordered to rule out urinary tract infection. The urine culture test showed sterile pyuria, with white cells >100 cells/uL (WCC 2+). No epithelial cell was detected and the bacteria count from the urine sample was insignificant (<10^4 cfu/mL).To work up the cause of sterile pyuria, early morning urine tests for mycobacterial culture and acid-fast bacilli smear were ordered. Two samples showed the presence of Mycobacterium tuberculosis, with one sample showing positive acid-fast bacilli smear. The cause of proteinuria and sterile pyuria for this patient was urological tuberculosis. The patient was called back for further assessment. The contact history of tuberculosis was traced. Her husband had pulmonary tuberculosis more than 10 years ago. She was screened as a close contact at that time, with a chest X-ray done, and the result was unremarkable. She revealed that she had cough, subjective weight loss, and occasional haemoptysis in the past few months. She also mentioned that she had an abnormal chest X-ray in 2017. However, she did not seek medical help after she received the result. The private chest X-ray in 2017 showed the presence of a 1.5 x 1.5cm radiopaque pulmonary nodule at the left lower lung. A chest X-ray was arranged. The repeated chest X-ray also showed a 1.6cm radiopaque nodule at the left lower zone of the pericardial region. Bronchial dilatation with bronchial wall thickening at the right lower zone was also detected, suggesting bronchiectasis or bronchitis. To rule out concomitant pulmonary tuberculosis, a sputum test for mycobacterial culture was ordered. Sputum culture was negative for Mycobacteria tuberculosis. To delineate the nature of the lung nodule, Computed Tomography (CT) thorax was arranged. CT thorax suggested that the lung nodule was an old fibrotic granuloma. Findings secondary to old tuberculosis were present in the CT examination, including diffuse parenchymal scarring in all the lobes of her lungs, old reactive lymph nodes in the mediastinum and pulmonary hila, and tractional bronchiectasis. The patient was diagnosed to have urological tuberculosis with concomitant culture-negative pulmonary tuberculosis. She was referred to the urology clinic for further investigation and was referred to the chest clinic (Department of Health) for antituberculous medications. A CT abdomen and pelvis was ordered to look for complications of urological tuberculosis in the urinary system. It revealed the presence of left hydronephrosis. Left ureteroscopy was performed and this detected a 1cm left L2/3 ureteric stricture. Irregular contour over the left distal ureter was also detected, from the vesicoureteric junction to the lower border of her sacroiliac joint. A biopsy was taken which confirmed the presence of granulomatous inflammation. As for the anti-tuberculous medications, she needed to complete a1-year course as she had both extra-pulmonary and concomitant pulmonary tuberculosis.
DiscussionSterile pyuriaSterile pyuria is defined as the absence of bacteria, with the presence of 10 or more white cells per microliter (μl) in a urine specimen.1 Differential diagnoses of sterile pyuria include infectious and non-infectious causes. Details are listed in Table 1. Infectious causes include recently treated urinary tract infection, sexually transmitted infections and urinary tract infections by atypical organisms. For an immunocompromised patient, atypical infections caused by Mycobacterium tuberculosis and fungi need to be considered. If no infections were to be are detected after further investigations, one could then consider non-infectious causes if the patient is symptomatic. 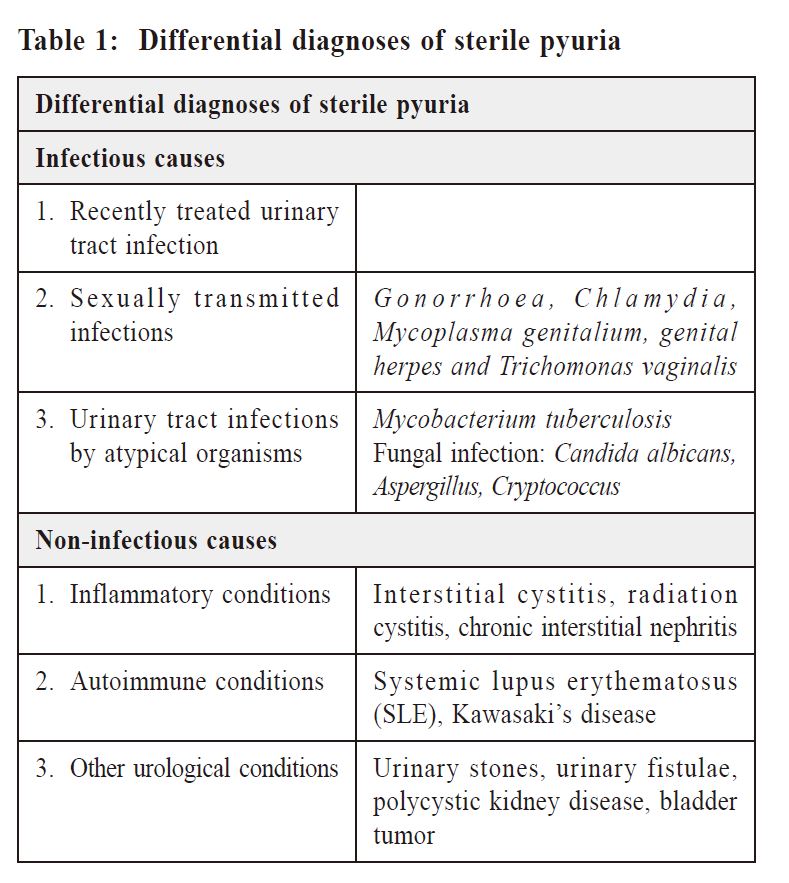
Urological tuberculosis Urogenital tuberculosis is a neglected clinical problem, owing to its non-specifics symptoms, insidious onset, and lack of clinicians’ awareness of the possibility of tuberculosis. This commonly leads to a delay in diagnosis which could result in disease progression and complications. Urogenital tuberculosis is the third most common form of extra-pulmonary tuberculosis, after lymph node involvement and tuberculous pleural effusion. It can occur in 2-20% of patients with pulmonary tuberculosis. Risk factors for this patient include diabetes mellitus and a history of contact with tuberculosis. Urological tuberculosis is generally more common among immunocompromised patients in a region with a high incidence of tuberculosis. Mycobacterial seeding of the urological tract is via haematogenous or lymphatic spread. It could occur at the time of primary pulmonary infection or in the setting of reactivation of tuberculosis and miliary tuberculosis. If left untreated, the tuberculous infection can lead to complications such as renal abscess, urethral stricture, hydronephrosis, renal dysfunction, and bladder fibrosis.2 Clinical manifestations of urological tuberculosis are quite non-specific. Patients usually presented with incidental findings of sterile pyuria or microscopic haematuria. For the more severe case with involvement of the bladder, they may present with frequency of urination, dysuria, gross haematuria, or loin pain. If patients have concomitant pulmonary tuberculosis, they could have systemic symptoms such as fever, weight loss, or night sweat. 
Urological tuberculosis is diagnosed by the detection of Mycobacterium tuberculosis in a urine culture. The specificity of this test is 100%. As the number of tuberculous bacilli in urine is relatively small, this could lead to a low sensitivity, and hence it is recommended to save three to six early morning urine samples if feasible. For patients with suspected urological tuberculosis, but with negative urine culture, imaging via CT with contrast is recommended. Evidence of stricture through out the collecting system, renal scarring, calcification throughout the urinary tract and hydronephrosis may suggest urological tuberculosis. Renal and bladder biopsy may be needed for microbiological or histological examination of tuberculosis. The treatment of urological tuberculosis is similar to pulmonary tuberculosis, with the use of a combination of anti-tuberculosis medications. The infectivity of tuberculosis is reduced significantly after two weeks of effective anti-tuberculosis treatment.3
ProgressAfter our patient was diagnosed with urological tuberculosis and concomitant pulmonary tuberculosis, she came back for regular follow-ups for her chronic conditions. During one of her follow-ups, she reported that her urinary symptoms had resolved with antituberculosis treatment. She had also gained some weight. She appeared relieved. I spent some time exploring the meaning of her diseases to this patient. This patient had diabetes mellitus and hyperlipidaemia and was on diet control only, yet she came back for follow-up every four months for around four years. However, she did not seek medical help for her abnormal chest X- ray. I did not understand why she did not take further action after the discovery of the lung nodule. The patient explained that she thought she had lung cancer. In her view, lung nodule meant cancer, and cancer meant an incurable disease. She decided to ignore the “cancer” and just let it be. She was afraid that her family members would spend lots of money on her treatment once they knew that she had cancer. The reason she came for the follow-up is that she thought she could do something actively to improve hyperlipidaemia and diabetes mellitus.In family medicine, emphasis is on the importance of good communication skills. In a consultation, we often explore the patient’s ideas, concerns, and expectations. Patients can convey lots of information in a consultation. It is very important that we listen well and grasp their main concerns and offer patientcentered management. “To listen well is to figure out what’s on someone’s mind and demonstrate that you care enough to want to know.”4 Through listening, we could understand our patients more. After understanding more about our patients, we could be more empathetic and connected to them.
ConclusionFor a patient with symptomatic sterile pyuria, we should order further investigations to rule out other causes, especially urological tuberculosis. Referencess
Esther SC Pang,
MBBS (HKU), FHKCFP, FRACGP
Correspondence to: Dr. Esther SC Pang, 10 Aberdeen Reservoir Road, Aberdeen,Hong Kong SAR.
|
|