
|
June 2023,Volume 45, No.2
|
Case Report
|
Secondary periodic paralysis in a lady following newly diagnosed hypertensionFang-fang Jiao 焦芳芳, Derek GC Ying 刑格政, Catherine XR Chen 陳曉瑞 HK Pract 2023;45:53-56 SummaryWeakness and fatigue are one of the most common yet vague complaints encountered by primary care physicians. These complaints are usually nonspecific, and may represent a plethora of medical, psychiatric, or even social conditions. Periodic paralysis (PP) is one of the rarer causes of limb weakness. If given detailed history taking, laboratory investigations and diagnostic awareness, it can be timely diagnosed and properly managed at primary care level. Here we present the diagnostic process of a case of secondary PP in a lady with recently diagnosed hypertension. Keywords: Periodic paralysis, hypokalaemia, thiazide diuretics, primary care
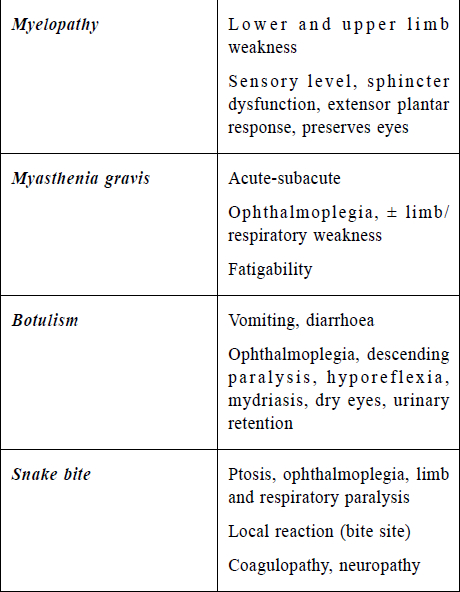
摘要疲勞無力是基層醫生最常見但是模糊不清的主訴之 一。這個主訴雖然不明確,但是可以由很多生理,心理甚 至社會性的原因引起。週期性麻痹是肢體無力的一個罕見 原因,但是通過詳盡的病史採集,實驗室檢查和診斷警 覺,這個疾病可以在基層醫療得到及時診斷和良好醫治。 本文描述了一位新確診高血壓的女士患有週期性麻痹的診 治過程。 關鍵詞: 週期性麻痹,低鉀血症,噻嗪類利尿劑,基層醫療 The CaseMadam A, a 68-year-old lady, is a non-smoker and non-drinker. She attended a General Out-patient Clinic (GOPC) of the Hospital Authority (HA) of Hong Kong on 19th March 2021 for sudden onset of limb weakness for two weeks. The weakness involved all four limbs and was symmetrical in distribution. During the attack, the patient was unable to get up from a chair or raise up her arms. It occurred recurrently and intermittently, with 1-2 episodes per day and each episode lasting for 15 to 30 minutes. The condition was associated with sense of fatigue and usually resolved spontaneously and completely after each episode. Otherwise, there was no limb numbness, facial asymmetry or slurred speech. She had no palpitation, hand tremor or weight changes either. There was no preceding hunger, sweating or dizziness, nor did she have any vomiting or diarrhoea lately. She had no similar attacks of limb weakness before. Further history taking revealed that she attended her private general practitioner on 5th March 2021 to assess the fitness for COVID-19 vaccination. During that clinical visit, she was newly diagnosed to have hypertension (HT) and subsequently was treated with Lercanidipine 10mg daily and indapamide 2.5mg daily for blood pressure (BP) control. She was advised not to receive the COVID-19 vaccine due to the unstable medical condition. The weakness happened after she took these anti-hypertensive medications. Otherwise Madam A enjoyed good past health and has not taken any medications or herbs from over the counter. Her mood was stable all along and she could cope with her daily life well. There is no family history of neurologic disorder. Physical examination on 19th March, 2021 showed satisfactory general condition and the gait was normal. There was no pallor or jaundice. Clinic BP was 136/86 mmHg, pulse was 93 beats per minute, regular. Hstix was 6.5 (mmol/L) (2h post prandial). Neurological examination showed normal power, sensation, muscle tone and reflex of all limbs. There was no facial weakness or asymmetry. Clinically Madam A was euthyroid and her mental status was neutral. As the patient was suspected to suffer from hypokalaemia periodic paralysis induced by indapamide use, she was advised to withhold indapamide immediately. Lercanidipine was changed to amlodipine 10 mg daily according to HA Drug Formulary. Blood tests on the same day (19th March 2021) showed serum potassium level was 3.0 (mmol/L), other laboratory results including serum sodium level, renal and liver functions, thyroid functions, complete blood picture and bone profiles were all normal. Urgent CT brain exam arranged in the private also revealed normal findings without vascular abnormalities or intracranial lesion. The patient was reviewed on 26th March 2021. The periodic weakness resolved after indapamide was off. Her clinic BP was 127/77 mmHg on amlodipine 10 mg daily. One week of Slow K 600 mg daily was prescribed for the correction of hypokalaemia. Subsequent blood test on 10th April 2021 showed normalised potassium levels of 4.1 mmol/L. DiscussionPeriodic paralysis (PP) is a rare group of muscular disorders characterised by recurrent episodes of hyporeflexia and skeletal muscle weakness, stiffness or paralysis lasting for minutes to days.1 The weakness typically involves the four limbs symmetrically, with proximal muscles more prominently affected. PP does not affect extra-ocular movements, swallowing, respiration, sphincter functions, cognition and sensory system.2 Apart from its effects on muscle strength, PP is associated with impairments of quality of life due to muscle weakness and fatigue, therefore may affect patients’ ability to participate in social and family life.3 PP is caused by malfunctioning of ion channel in skeletal muscles, with potassium abnormalities as its hallmark electrolyte disturbance. PP can be inherited (primary) or acquired (secondary). Primary PP syndromes, such as familial PP, are inherited in autosomal dominant pattern. It includes hypokalaemia PP, hyperaemic PP and Andersen-Tawil syndrome, with hypokalaemia PP being the most common form.4 Its onset can be triggered by strenuous exercise, certain foods (such as lots of carbohydrates with sugars and starches), stress and cold temperatures.1 The global prevalence of heritable hypokalaemia and hyperaemic PP are estimated to be 1:100 000 and 1:200 000 respectively.2 The onset typically occurs in the first or second decades, and the attacks may be mild or severe and may last for minutes or days.5 Diagnosis of primary PP is based on the characteristic clinic presentation and confirmed by genetic testing. Secondary PP usually refers to PP induced by hypokalaemia due to other aetiologies. It is more prevalent in elderly Asians with low potassium level, and presents with more prominent clinical symptoms and signs. Aetiologies include druginduced, thyrotoxicosis, renal tubular acidosis, primary hyperaldosteronism, gastrointestinal (GI) loss and viral infections such as Dengue. Less common causes include Cushing’s syndrome, Liddle’s syndrome, massive liquorice intake or congenital adrenal hyperplasia.3 Hypokalaemia PP (hypoPP) is defined as recurrent episodes of acute onset flaccid paralysis associated with low plasma potassium (<3.5 mmol/L). The condition should be suspected when a patient presents with recurrent attacks of sudden muscle weakness involving proximal muscles following identifiable triggering factors, such as strenuous exercise, consumption of diet rich in carbohydrates, stress, or other cause of hypokalaemia, such as diuretics use. When there is an established family history of hypoPP, no further diagnostic investigations are required to confirm the diagnosis. Otherwise, a low serum potassium level during a typical attack of weakness establishes the diagnosis.3,6 Neurological examination of the patient during attack shows generalised muscle weakness, hyporeflexia or areflexia but findings are usually normal between the attacks. If patients present atypically, or after their first episode of paralysis, other differential diagnoses, such as myasthenia gravis, Guillain-Barre syndrome, and myelopathy, should be considered.1 The differential diagnoses of other types of acute onset of paralysis are summarised in Table 1. In our case, madam A presented with recurrent episodes of acute limb weakness for two weeks. The character of the weakness was consistent with the features of PP. She did not have any clinical features suggestive of GI loss or renal loss, there were no symptoms suggestive of thyroid disorder or other endocrine abnormality. However, as weakness is such a common and nonspecific presentation in outpatient settings, stroke, brain tumour or other neurological conditions that may cause nerve entrapment and are potentially life-threatening should always be ruled out first. Thorough history taking, normal findings on the neurological exam, normal baseline blood investigations except hypokalaemia and normal brain imaging studies excluded the other differential diagnoses. In view that Madam A has no family history of neurological diseases and the late onset of PP at 68 years old, secondary PP was highly suspected. Her recent prescription of diuretics for the newly diagnosed HT rendered it very likely that indapamide induced hypokalaemia is the culprit of the attacks. Researchers are still investigating how low potassium levels may be related to the muscle abnormalities in this condition. One case study of 29 patients with hypokalaemia PP showed the serum potassium ranged from 1.2 to 3.1 mmol/L.3 Another study found the mean serum potassium to be 3.18±0.5 mmol/L among 18 patients with hypokalaemia PP.6 In our case, Madam A’s potassium level was 3.0 mmol when she was paralysis free. We suspect that her potassium level might be even lower during the paralysis attack. Madam A's potassium level was similar with those reported in previous case studies. Although low dose indapamide 2.5mg/day seldom cause significant hypokalaemia, severe hypokalaemia (plasma potassium concentrations of 1.6-2.2 mmol/L) have been reported after indapamide 2.5 mg/day for hypertension.7 In equivocal cases, genetic studies, electromyogram and provocative testing may provide additional evidence for diagnosis. Complications of hypokalaemia PP are rare, but clinicians should be aware of rhabdomyolysis and cardiac arrhythmia in severe cases.8 Treatments of PP include behavioural interventions directed at avoidance of triggers, modification of potassium levels, and the use of carbonic anhydrase inhibitors.9 Medical professional could begin with patient education on the nature of the condition and advise them on the lifestyle changes to minimise triggers of PP. Correction of hypokalaemia restores cell membrane polarisation, resulting in release of potassium stored in intracellular compartment and a rebound hyperkalaemia. As such, oral potassium supplementation is preferred over intravenous infusion to avoid rebound hyperkalaemia. Complete resolution of symptoms is expected after correction of potassium levels , as in our case. Carbonic anhydrase inhibitors (in particular acetazolamide and dichlorphenamide) have been used for almost 50 years as empiric treatment of PP but the mechanism of action is not completely understood.10 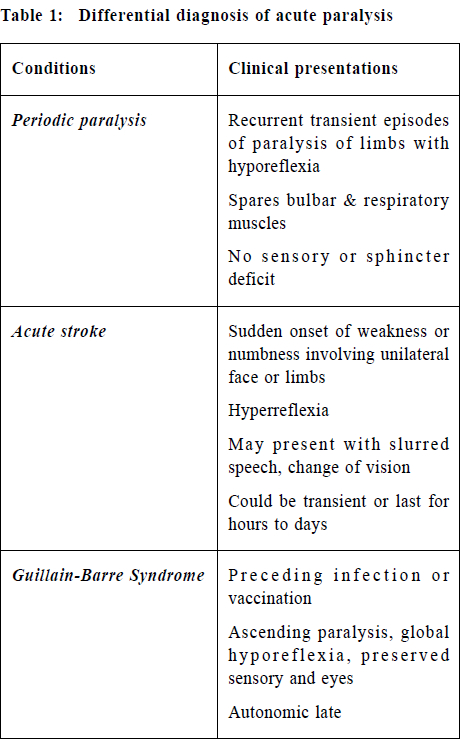
ConclusionPP is a group of rare neuromuscular disorders with hypokalaemia PP being its main type. Secondary hypokalaemia PP should always be considered as a differential diagnosis in patients presenting with acute onset of periodic muscle weakness over the limbs, especially when stroke and other severe neurological disorders are ruled out. Detail clinical and drug histories are essential in identifying the causes of hypokalaemia in secondary PP. Treatments of PP include behavioural interventions directed at avoidance of triggers, modification of potassium levels, and the use of carbonic anhydrase inhibitors. Complete resolution of symptoms is expected after potassium level is corrected. References
Fang-fang Jiao,
LMCHK, FHKCFP, FRACGP, PhD (Family Medicine, HKU)
Derek GC Ying,
LMCHK, FHKAM (Family Medicine), FRACGP
Catherine XR Chen,
LMCHK, FHKAM (Family Medicine), PhD (Medicine, HKU), MRCP (UK)
Correspondence to:
Dr. Fang-fang Jiao, Room 807, Block S, Dept of FM & GOPC,
|
|