|
June 2023,Volume 45, No.2
|
Update Article
|
Interpreting chest radiographsWilfred CG Peh HK Pract 2023;45:35-44
SummaryChest radiographs are a common, inexpensive and widely-available imaging modality that, when used appropriately, is effective in aiding clinical management. This article aims to provide a practical refresher for family physicians in the basic approach to interpreting chest radiographs and highlights technical considerations to be aware of. The radiographic appearances of some common entities such as cardiac failure, lung cancer, pneumonia, pleural effusion, pneumothorax, together with incidentalomas and artifacts, are reviewed.Keywords: Cardiac failure, chest incidentaloma, chest radiograph, lung cancer, pleural effusion, pneumonia, pneumothorax, radiographic artifact
摘要胸部X光檢查是常用便宜且被廣泛採用的影像學方式 ,若正 確的使用可以有效的幫助臨牀治療。本文目的在於幫助家 庭醫生重溫胸部X光的基本解讀,並著重說明分析某些常 見疾病的放射影像技術要點,包括: 心髒衰竭 ,肺癌,肺 炎,胸腔積液,氣胸,偶發瘤及人工假影。關鍵詞: 心髒衰竭,胸部偶發瘤,胸部光檢查,肺癌,胸腔 積液,肺炎,氣胸,人工假影 IntroductionChest radiographs are probably the most common medical imaging procedure performed. Compared to other more advanced imaging modalities, it is inexpensive, widely available, and easy to perform. It is effective in aiding clinical management, when utilised appropriately. However, chest radiographs have some inherent limitations and may need to be supplemented by other forms of imaging, e.g. computed tomography (CT) in certain circumstances. Most family physicians are expected to be able to interpret chest radiographs, in contrast to advanced forms of imaging such as CT and magnetic resonance imaging (MRI) where specialised radiologist expertise and experience is usually required. This article aims to provide a practical refresher for family physicians in the basic approach to interpreting chest radiographs and to review the appearances of some relevant common lesions. IndicationsListing all the specific indications for performing a chest radiograph is beyond the scope of this article. Details can be found in excellent referral guidelines/ appropriateness criteria published by professional bodies such as the Royal College of Radiologists1 and the American College of Radiology.2 In general, imaging is a powerful tool that supplements, but does not replace, a carefully-taken history and a thorough physical examination. Chest radiographs are usually indicated when the patient’s symptoms are suspected to be related to problems arising within the chest. Some of these symptoms include chest pain, persistent cough, fever and dyspnoea, resulting from conditions such as cardiovascular disease, pneumonia, lung and pleural malignancy, chronic obstructive pulmonary disease, pneumothorax and chest trauma. Table 1 lists some common indications for performing a chest radiograph.3 Like other imaging procedures that utilise X-rays, performing a chest radiograph carries a radiation risk. For a single posterior-anterior (PA) chest radiograph, the typical effective dose is 0.015mSv, which is approximately equivalent to 2.5 days of background radiation. This contrasts with head CT which has a typical effective dose of 1.8mSv (10 months of background radiation) and chest CT which has a typical effective dose of 14mSv (6.5 years of background radiation).4 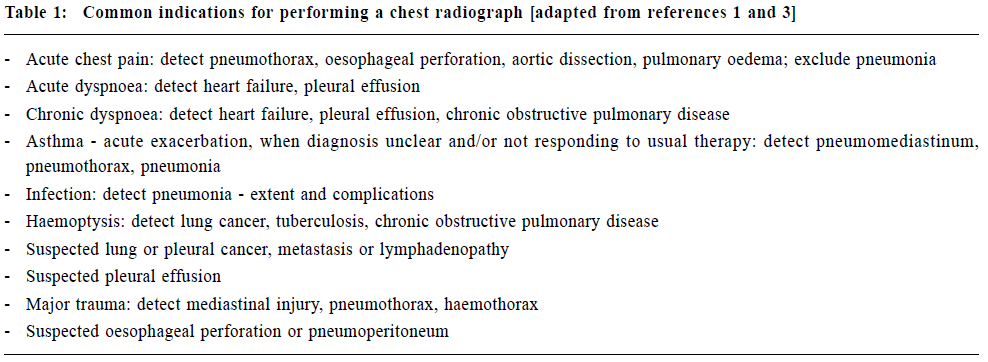
Although the radiation dose incurred is relatively small, requesting chest radiographs are still best avoided unless there are clear diagnostic benefits. Compliance with standard indications for various imaging procedures found in widely-accepted referral guidelines are therefore key to obtaining the necessary diagnostic information, while minimising ionising radiation hazard to your patients.1,2 Technical considerationsPrior to interpreting a chest radiograph, there are a few technical factors to consider. This is important as failure to appreciate these factors may have an impact on the accuracy of your interpretation. Questions to ask yourself:
Approach to interpretationEmploy a systematic approach so that you will not miss any lesion. Having a checklist is useful, even though in normal clinical practice, you will probably already have a working diagnosis based on history and physical examination findings. By the time your patient goes for a chest radiograph, you will already be looking to confirm your clinical suspicions by the expected detection or exclusion of certain lesions. My own system is to:
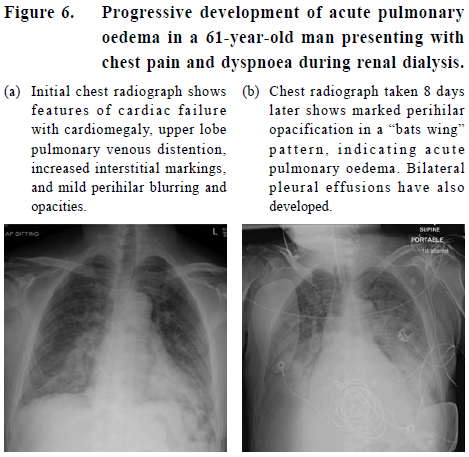
Common lesionsIn this section, I have listed a selection of common lesions which I feel are relevant to family physicians. These are entities that may be encountered in the course of a community-based practice, and would be quite different from the pattern of lesions found in an acute hospital setting. In cardiac failure, the heart is enlarged, with a CTR exceeding 0.5. Left ventricular failure results in pulmonary venous distention in the upper lobes. Increased pulmonary venous pressure causes pulmonary oedema which manifests as blurring of the hilar vessels and perihilar opacification (Figure 5 & 6). This is followed by development of pleural effusions and septal lines at the costophrenic angles. The finding of 1-2cm long, 1mm thick horizontally-oriented septal lines in both costophrenic angles indicate early interstitial pulmonary oedema. Further progression of cardiac failure may result in acute pulmonary oedema, producing a “bats wing” distribution of prominent perihilar opacification (Figure 6). 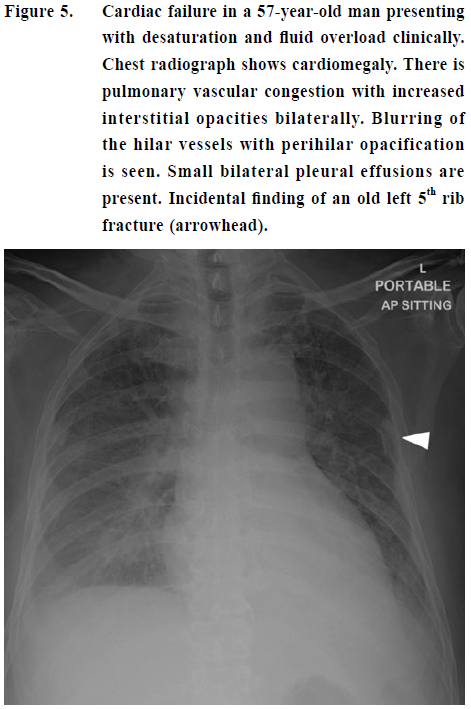
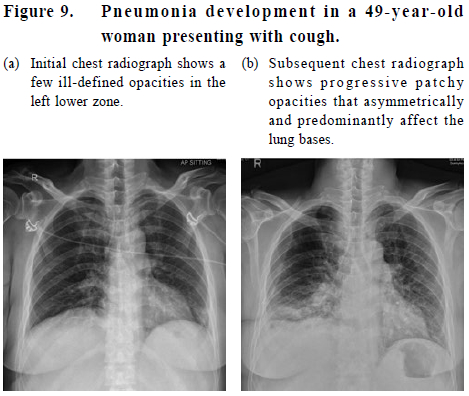
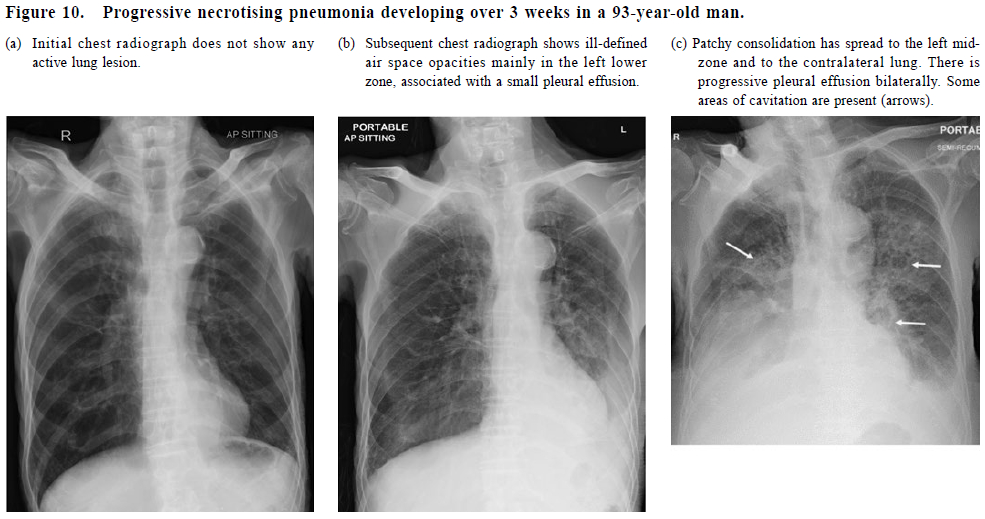
Lung cancer often manifests as a solitary pulmonary nodule larger than 3cm in diameter (Figure 7). Lung cancer may also be seen as a hilar mass when the cancer arises from a proximal bronchus, with associated tracheobronchial lymph node enlargement. Sometimes, the adjacent airway is obstructed by the tumour, with resultant lobar or segmental collapse. A Pancoast tumour involves the apex of the lung and is typically difficult to detect due to overlying bony structures. Addition of an apical view radiograph helps better demonstrate this tumour (Figure 8). Pulmonary metastases typically present as multiple well-defined rounded lung masses. Pneumonia is seen as air space opacification (or consolidation) due to filling of the pulmonary alveolar air space by inflammatory exudate from the infection. Patterns of pneumonia include lobar pneumonia when it is confined to one lobe, and bronchopneumonia. The latter is characterised by multiple small nodular or reticulonodular opacities which tend to be ill-defined, patchy and/or confluent. The adjacent pulmonary vessels are typically obscured. The distribution is often bilateral and asymmetrical, predominantly affecting the lung bases (Figure 9). When there is extensive necrosis of lung tissue, cavities may form, producing a cavitating or necrotising pneumonia (Figure 10). Aspiration pneumonia occurs when food or liquid is breathed into the airways or lungs, instead of being swallowed (Figure 11). In an erect patient, aspiration is more likely to involve bilateral lower lobe basal segments and the middle lobe. In a supine patient, the posterior segment of the upper lobes and the superior segment of the lower lobes are the most commonly involved sites. 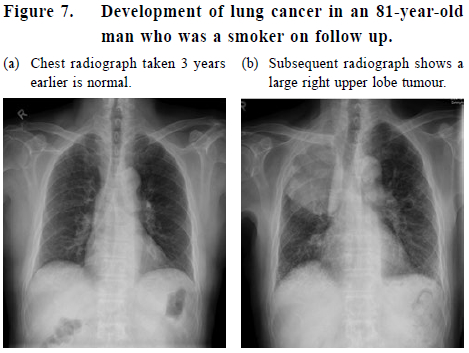
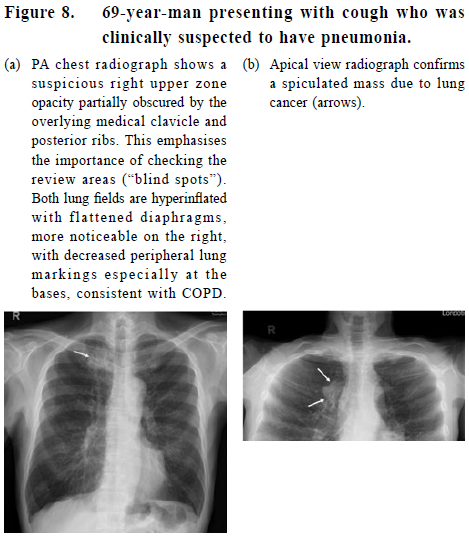
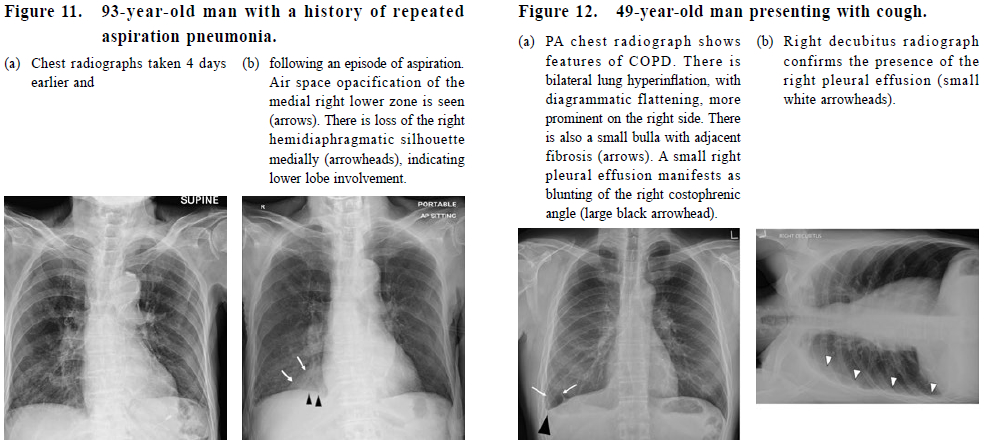
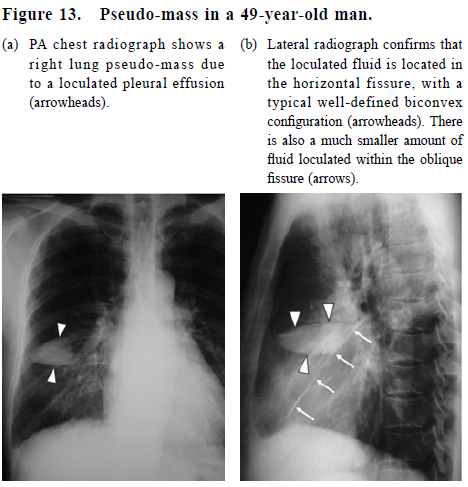
Chronic obstructive pulmonary disease (COPD) includes two key components, namely: chronic bronchitis with airflow obstruction and emphysema. Patients may have airways-predominant or emphysemapredominant disease, or a mixed pattern. The most common risk factor is cigarette smoking. In general, chest radiographs have a poor sensitivity for detecting COPD but helps support the diagnosis in more severe disease. Radiographic features include lung hyperinflation with a flattened diaphragm, bulla formation, bronchial wall thickening, hyperlucent lung due to parenchymal loss and decreased peripheral lung markings (Figure 8 & 12a). Pleural effusion refers to abnormal accumulation of fluid within the pleural space and is usually detected as blunting of the costophrenic angle on the chest radiograph (Figure 5, 6, 10 & 12). It is generally acknowledged that as much as 250-300ml of pleural fluid may be present before it is visible radiographically. A subpulmonic collection of pleural fluid may manifest as apparent elevation of the hemidiaphragm, although a clue is that the ipsilateral costophrenic angle is almost always blunted. Adding a lateral decubitus radiograph helps confirm the presence of a pleural effusion (Figure 12b). Sometimes, pleural fluid is loculated in a fissure, appearing as a pseudo-mass which may be mistaken for a lung tumour (Figure 13). A lateral radiograph is useful to delineate the orientation and course of the fissure, particularly if it contains pleural fluid. Many different pathological processes can produce pleural effusions, which can in turn be broadly divided into transudates and exudates. While pleural effusions are usually easily detected, the different fluid types cannot be distinguished radiographically.
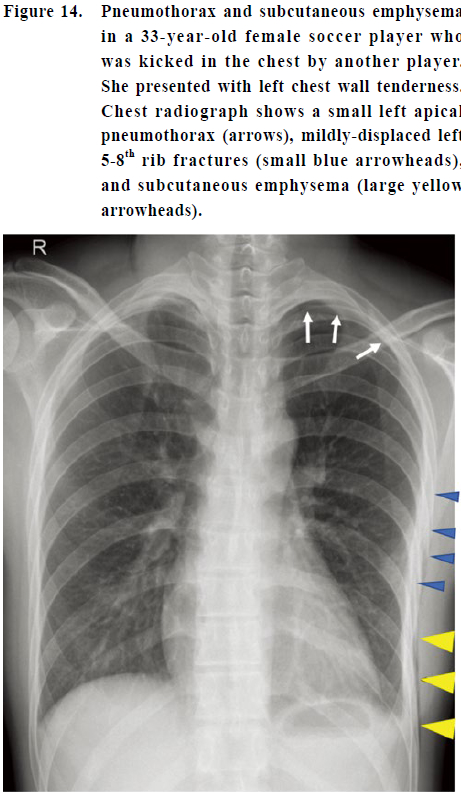
Pneumothorax refers to the presence of gas in the pleural space. This is best seen at the apical region on a PA erect chest radiograph as a thin white line representing the visceral pleura being separated from the chest wall, with absent lung markings peripheral to this line. This peripheral space is typically hyperlucent compared to the adjacent lung. A small pneumothorax can easily be missed unless it is looked for (Figure 14). A large pneumothorax can produce collapse of the underlying lung or progress to a tension pneumothorax, with resultant life-threatening haemodynamic compromise. Hence, early detection of a pneumothorax is important. A pneumothorax may occur spontaneously (with or without underlying lung disease) or secondary to trauma or iatrogenic injury. In young persons with bronchial asthma, spontaneous pneumothorax is one of the complications to look out for. Sometimes, there is an associated subcutaneous emphysema or pneumomediastinum. Subcutaneous emphysema refers to the presence of gas in the loose subcutaneous areolar tissue and/or muscle, and produces a characteristic linear streaky hypodensity radiographically (Figure 14). A pneumomediastinum refers to the presence of extraluminal gas within the mediastinum, and appears radiographically as a linear or curvilinear hyperlucency outlining the mediastinal contours (Figure 15). There are a variety of aetiological factors, and the gas can track from various structures such as the lungs, trachea, oesophagus and even the peritoneal cavity.
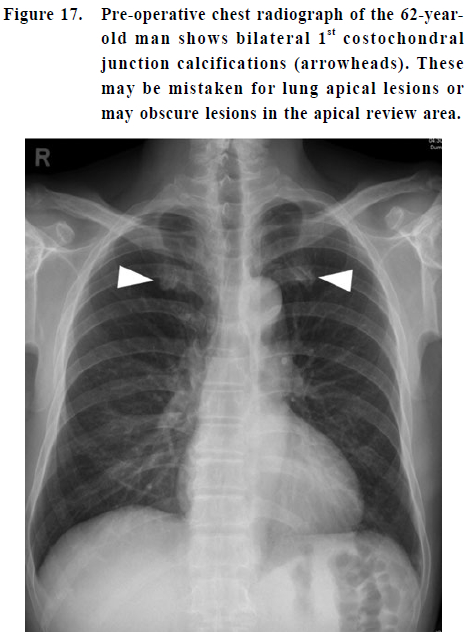
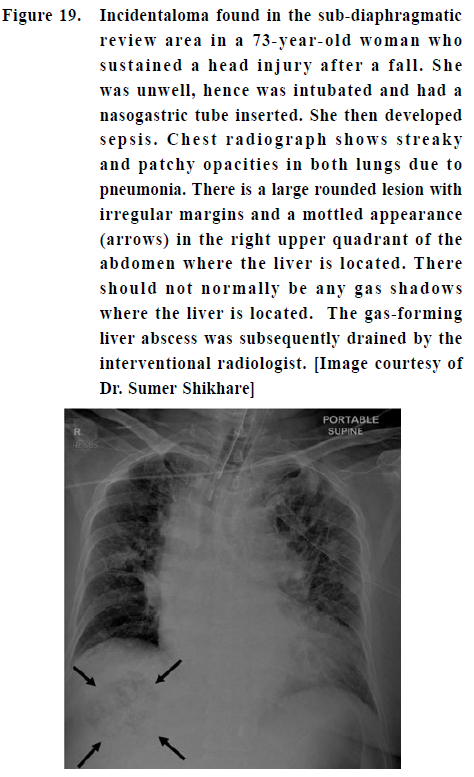
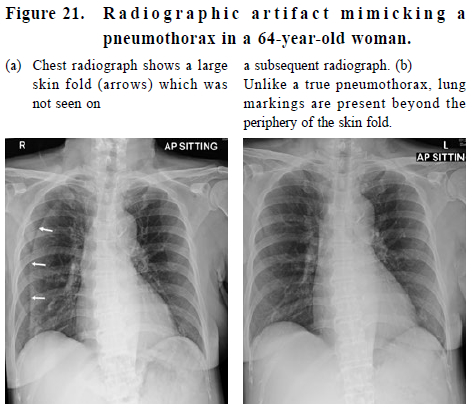
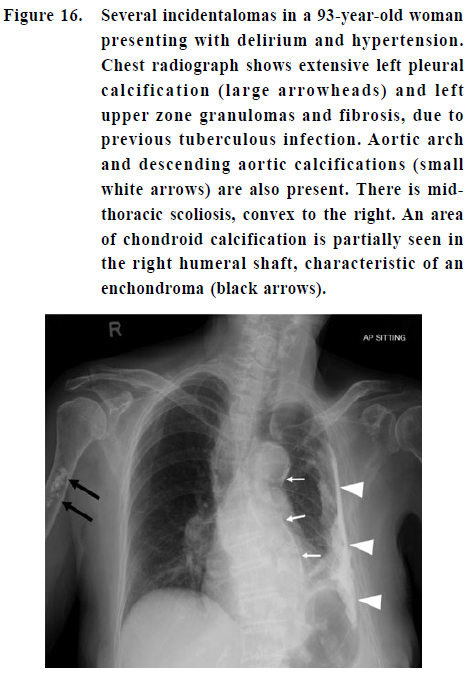
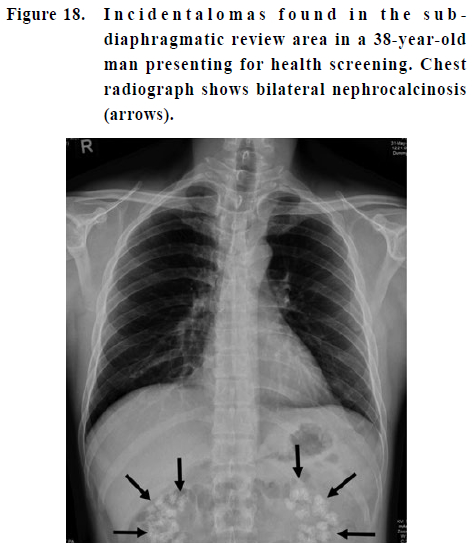
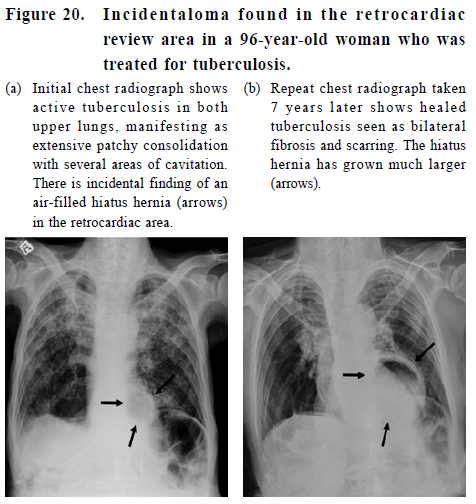
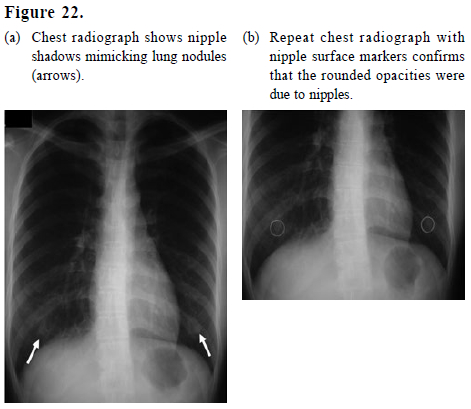
An incidentaloma is a radiological term used to refer to a lesion found incidentally. Although usually detected in asymptomatic patients, some may be clinically significant and need further workup; while the presence of others may interfere with diagnostic interpretation. Bony incidentalomas include vertebral anomalies, tumours and costochondral calcifications or osteoarthritis (Figure 16 & 17). Soft tissue incidentalomas include lesions arising from the viscus e.g. hiatus hernia or abdominal organs e.g. nephrocalcinosis, gas-forming liver abscess, emphasising the importance of paying attention to the review areas (sub-diaphragmatic and retrocardiac “blind spots”) (Figure 18-20). Finally, there are a host of normal structures that may produce radiographic artifacts, mimicking lung lesions. These include seeminglyharmless structures such as skin folds and nipples (Figure 21 & 22)! For clearly benign incidentalomas, they should be left alone and nothing further needs to be done. For incidentalomas of potential clinical significance, the suggested course of action would be for the family physician to clinically assess the patient in the light of the unexpected new finding and if warranted, refer to the relevant clinical specialist. Some parting thoughtsA Dutch study on the influence of both positive and negative chest radiographic findings in general practice found that patient management changed in 60% of patients following chest radiographs. Chest radiographic findings substantially reduced the number of specialist referrals, a reduction in number of patients with initiation or change in therapy, and more frequent reassurance of patients. This study concluded that chest radiographs are an important diagnostic tool for general practitioners.5 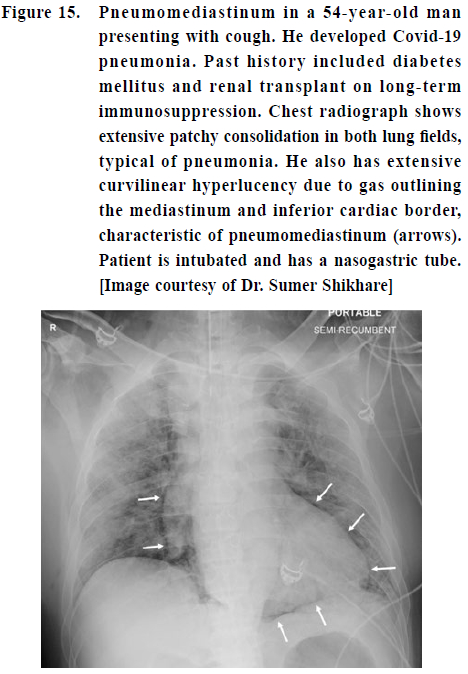
The chest radiographic findings should always be reviewed in the context of the clinical features (history and physical examination). Many lesions in the lungs may have a similar appearance e.g. a lung opacity may be due to tumour, infection, trauma (contusion or haemorrhage), infarction or fluid overload. The clinical context and available laboratory results are therefore key to distinguishing among the various possible aetiologies. After requesting a chest radiograph for your patient, it is the referring clinician’s duty of care to follow-up the results promptly, i.e. review the radiologist’s report. As the radiologist may not have adequate or relevant clinical information, the report may not always answer the specific clinical question sought. If there is any doubt regarding a report, I would strongly recommend that the referring clinician contacts and communicates with the radiologist. This scenario will only arise if the family physician is comfortable with and has the practice of reviewing and interpreting their patient’s chest radiographs personally. AcknowledgementI thank Dr. Sumer Shikhare, Consultant and Chief, Cardiothoracic Imaging, Department of Diagnostic Radiology, Khoo Teck Puat Hospital, for his helpful comments. References
Wilfred CG Peh,
MD (Hong Kong), FRCPG, FRCPEd, FRCR
Correspondence to: Professor Wilfred CG Peh, Senior Consultant, Department of
Diagnostic Radiology,
|
|