
|
March 2023,Volume 45, No.1
|
Discussion Paper
|
Preconception care for women with pre-existing medical diseasesSue ST Lo 羅善清 HK Pract 2023;45:4-8 SummaryPreconception care is defined as the provision of biomedical, behavioural, and social health interventions to women and couples before conception occurs. It is about embedding principles and actions into current care models prior to first and subsequent pregnancies, and its objective is to improve couple’s health during their life course, minimise obstetric risks and optimise the development of their foetuses. This article illustrates how family physicians can provide preconception care and advice during their usual care for women with pre-existing medical diseases. Keywords: Obesity, Family physicians, Primary care
摘要孕前保健是指在婦女懷孕前向她及其伴侶提供身心、行 為和生活的改善建議, 以達致提升健康, 減低孕期風 險,及優化胎兒發育的目標。本文解構了家庭醫生如何 把孕前保健融入日常的診症中,為有基礎病的婦女提供 適切的孕前準備建議。 關鍵詞: 肥胖,家庭醫生,基層醫療 IntroductionGiving every child the best start in life is the priority of every parent. This is particularly important for women with pre-existing medical diseases because maternal and foetal wellbeing can be compromised by their illness and drug treatment. According to the service statistics of the Family Planning Association of Hong Kong (FPAHK), the top five pre-existing medical diseases among women attending their Prepregnancy Preparation Service are (in order) thyroid diseases, depression, asthma, epilepsy, and systemic lupus erythematosus (SLE). Preconception care aims at minimising maternal morbidity and optimising the epigenetic environment for the developing foetus. There is evidence to support preconception interventions improve maternal and neonatal outcomes.1 Preconception care is different for each person. This is a person-centred, holistic care that helps women plan their best time to conceive, optimise their fitness for pregnancy, live well and stay healthy. Family physicians have a key role in assisting couples to identify preconception risks and help them make informed decisions about planning or avoiding pregnancy. No one expects an unplanned pregnancy, but it happens often. If a family physician determines that pregnancy is risky for a woman with a pre-existing medical disease because the disease is poorly controlled or a potentially teratogenic drug cannot be suspended, effective contraceptives should be provided to avoid an unplanned pregnancy. Planning pregnancyThe median age of first childbirth in local women has steadily increased from 28.1 to 32.6 years old between 1991 and 2021.2 Therefore, the demand for infertility treatment and high-risk obstetric care required by older moms will not abate in the near future. To reduce such burden on the public healthcare system, couples should be encouraged to plan parenthood once they get married. They need to decide on the number of children they want, the timing of conception, the spacing of pregnancies and which contraceptive to use. Women with pre-existing medical diseases should be informed about the effect of their diseases and treatment on pregnancy and the developing foetus, and vice versa. Controlling medical illnessFor women with pre-existing medical illness, choosing the best time to conceive is particularly important. As a general rule, the best time to conceive is the time when the disease is in remission, or when it is well-controlled with medications which are compatible with pregnancy. Uncontrolled diseases can increase risk of medical as well as obstetric complications and compromise foetal development. This is particularly important for diseases like SLE, hyperthyroidism and type 1 or 2 diabetes mellitus. A systematic review and metaanalysis of observational studies of preconception care for women with pre-existing diabetes has demonstrated that receiving such care resulted in lower maternal HbA1c levels during their first trimester and a reduction in congenital malformations, preterm delivery, perinatal mortality, and neonatal intensive care unit admission.3 The glycaemic target suggested by the American Diabetes Association is HbA1c <6.5%, to reduce the risk of congenital malformations, preeclampsia, macrosomia, preterm birth, and other complications.4 Adjusting medicationsWhen a family physician treats reproductive age women, one should always be aware of the possibility of pregnancy and avoid teratogenic drugs. When no alternatives are available, teratogenic drugs such as isotretinoin, valproate and phenytoin can be used if the benefits of treatment outweigh the risks. These women need to understand the teratogenicity of the treatment and agree to use highly effective contraceptives.5 Patients should be encouraged to discuss the timing of their pregnancy so that the family physician can try to stabilise their disease with less teratogenic drugs before they conceive. For the treatment of hyperthyroidism, propylthiouracil should be used instead of carbimazole. SLE patients should stop mycophenolate mofetil, cyclophosphamide, methotrexate, and thalidomide at least three months before contemplating pregnancy.6 Serotonin-norepinephrine reuptake inhibitors (SNRIs) like venlafaxine (Effexor) are associated with more birth defects than selective serotonin reuptake inhibitors (SSRIs) like sertraline (Zoloft), fluoxetine (Prozac) and paroxetine (Paxil). Escitalopram (Lexapro) is the SSRI with the lowest number of birth defects reported.7 Choice of antidepressant is based on shared decision making with your patients, taking into account the safety, effectiveness, differences in disease severity, relapse risk and the patient’s experience, etc. There is no single best drug. Detailed information regarding teratogenic drugs or drugs with potential teratogenic effects is available from the UK teratogenic information service website (www.uktis.org). The US Centers for Disease Control and Prevention (CDC) Treating for Two Initiative (https://www.cdc.gov/pregnancy/meds/treatingfortwo/ index.html) also provides useful guidelines and recommendations in helping physicians and women identify the safest treatment options for common conditions before, during, and after pregnancy VaccinationCongenital rubella syndrome, influenza, and hepatitis B infection are all vaccine-preventable diseases which can lead to poor maternal and neonatal outcomes.8 Although the rubella vaccination has been included in the local childhood immunisation program since 1978, 5.5% of women attending the FPAHK Premarital Check-up and Prepregnancy Preparation Services tested negative for the rubella antibody in 2021. In these cases, non-immunise women are offered immunisation and are reminded to avoid becoming pregnant until one month after vaccination.9 Women contemplating pregnancy should also consider vaccination against COVID-19 and seasonal flu. Hepatitis B vaccination should be provided to non-immunise women who work in the healthcare sector or whose partner is a carrier. According to the CDC, COVID-19 and hepatitis B vaccination started before pregnancy can be safely completed even if the woman gets pregnant subsequently.
Fitness for pregnancyUnhealthy behaviours are usually established well before pregnancy, thus early intervention at the start of reproductive years could help to mitigate preconception risks, promote fitness for pregnancy, and improve overall health and wellbeing. A universal, life-course approach helps women adopt healthy lifestyle choices such as having a balanced diet, regular exercise, and maintaining emotional wellbeing. These lifestyle modifications not only promote fitness for pregnancy but are also important adjuncts to disease management in women with chronic illness. DietLocal studies had shown inadequate dietary intake of iodine10,11, Vitamin D12, fibre, calcium and iron13 among reproductive age women. The FIGO Nutrition Checklist14 is a validated clinical practice tool that assists physicians in collecting baseline information on pre-pregnant weight and nutritional status and identifying nutritional issues that require attention. The checklist on the front page consists of four sections, with questions on specific dietary requirements, body mass index, diet quality and micronutrients. On the back page, there are guidance notes to aid the physician in interpreting the responses and providing counselling. Using this Checklist, Tsoi et al found that 95% of healthy pregnant women in early pregnancy recruited at their first antenatal visit reported at least one out of six suboptimal dietary practices.15 There was ample evidence to support the importance of maternal nutrition on long-term non-communicable disease risk for mothers as well as for future generations.14,16 SupplementationThere is conclusive evidence that periconceptional folic acid supplementation prevents the first occurrence17 and recurrence18 of neural tube defects (NTD). For women at low risk, they should start 0.4mg folic acid daily 2-3 months before conception and continued to 12 weeks’ gestation.19,20 For high-risk women, i.e. those who had previous affected babies and those on anti-epileptic drugs, the American College of Obstetricians and Gynecologists19 recommends 4mg folic acid daily while the Royal College of Obstetricians and Gynaecologists (RCOG) 20 recommends 5mg. The RCOG also recommends 5mg folic acid daily for women or partners who have NTD, women who have celiac disease, diabetes mellitus and those with BMI ≥30kg/m2.20 In Hong Kong, only 5mg folic acid tablets are available (https:// www.drugoffice.gov.hk/eps/do/en/doc/Compdium.pdf). Targeted supplementation should be given to meet specific needs of individual women. Complete blood count is usually taken for preconception assessment and those with iron deficiency anaemia should be given iron supplementation. Correction of anaemia before pregnancy and in the first trimester reduces the risk of preterm delivery and low birth weight babies.21 The Department of Health recommends educating women on adequate iodine intake during preconception to ensure optimal maternal thyroid function to support thyroid and neurodevelopment in the fetus.10 Women without thyroid disease, who do not consume adequate iodine from food to meet the daily requirement of 250μg should consider iodine supplementation during pregnancy and lactation.10 To date, no observational studies with large sample size or randomised controlled trials have been published on preconception iodine status or effect of iodine supplementation. In women with pre-existing thyroid diseases, excessive iodine supplementation may worsen their diseases. Other dietary or vitamin supplementations have not been shown to improve maternal or foetal outcomes.20 Weight optimisationWeight optimisation is important before pregnancy because overweight and obese women experienced an increased risk of miscarriage, gestational diabetes, gestational hypertension, preeclampsia, and caesarean delivery compared to normal weight women.22,23 Besides, babies born to overweight and obese mothers were at an increased risk of being admitted into the neonatal intensive care unit, macrosomia, and stillbirth.24 One study showed a 10% reduction in preconception BMI in overweight and obese women reduced the risk of gestational diabetes, preeclampsia, large for gestational age, an APGAR score below 6 at 5 minutes, and admission of both mother and baby to the intensive care unit by 15%.25 On the other hand, being underweight during the preconception period increases the risk of infertility, miscarriage, preterm birth, and small for gestational age babies.26-28 Therefore, helping women optimise their weight before pregnancy not only improves their fertility potential, it can also improve their maternal and perinatal outcomes. ExerciseWomen without contraindications (e.g. pre-existing cardiopulmonary diseases, antepartum haemorrhage, pre-eclampsia) should maintain an active life before, during and after pregnancy. Any forms of mild to moderate intensity aerobic exercises such as swimming, brisk walking, stationary bicycling, modified Yoga and modified Pilates improves heart-lung function, boost mood and prevent overweight. Avoid exercises that can cause injury such as contact sports, skydiving, hot Yoga, hot Pilates, scuba diving, skiing, surfing, etc. Avoid risk factorsPrepregnancy risk factors include smoking, alcohol, and substance abuse. Family physicians should encourage women to stop or avoid such behaviours before they conceive. Foetal alcohol spectrum disorders are a group of physical, behavioural, and learning problems that can occur in a person who was exposed to alcohol before birth. There is no known safe amount of alcohol use before or during pregnancy. All types of alcoholic beverages are harmful, including beer and wines. Cigarette smoking reduces fertility in both men and women.29 Although smoking is not teratogenic, it increases the risk of placenta previa, abruptio placentae, intrauterine growth retardation, low birth weight, and perinatal mortality.29 Therefore, men and women who plan to conceive should stop smoking. According to the 2021 data from the Central Registry of Drug Abuse, heroin, methylamphetamine (ice), and ketamine were the top three illicit drugs used by females aged 21 and over in Hong Kong (https://www.nd.gov.hk/statistics_list/doc/en/t15.pdf). The use of illicit drugs is associated with pregnancy complications, low birth weight, infant mortality, and neonatal abstinence syndrome.30 Any woman of a reproductive age who is using illicit drugs should be referred to drug rehabilitation programs for treatment and encouraged to use reliable contraception to prevent any unplanned pregnancy. Prevent foetal anomalyWith the advancement in genomic sequencing, carrier screening can be offered to individuals or couples to screen for over 100 types of autosomal recessive or X-linked genetic disorders regardless of ancestry and geographic origin. Preconception screening is recommended over prenatal screening since it may be less stressful on individuals who are tested positive.31 If both partners are found to be carriers of a genetic condition, they should be referred to clinical geneticists for counselling on their risk of having an affected child and their reproductive options such as donor sperm / egg, preimplantation genetic diagnosis with implantation of only unaffected embryos, prenatal diagnosis during pregnancy, adoption or remaining childless. In a local study of 123 Chinese women who underwent carrier screening, 56.1% of them were found to be carriers of at least one disease and 47.6% were carriers after excluding thalassaemias. The five most common diseases found were GJB2-related DFNB1 nonsyndromic hearing loss and deafness (1 in 4), alpha-thalassaemia (1 in 7), 21-hydroxylase deficient congenital adrenal hyperplasia (1 in 13), beta-thalassaemia (1 in 14), and Pendred's syndrome (1 in 36).32 
ConclusionFamily physicians play a key role in delivering preconception care to women with pre-existing medical diseases. They should be aware that women of reproductive age can be pregnant at any time, hence they should warn women against pregnancy when their disease is not under control, avoid teratogenic investigations and treatment if possible, and regularly review the women’s lifestyle. Encouraging women to adopt “clean and healthy living” during the preconception period helps to optimise maternal and foetal outcomes. 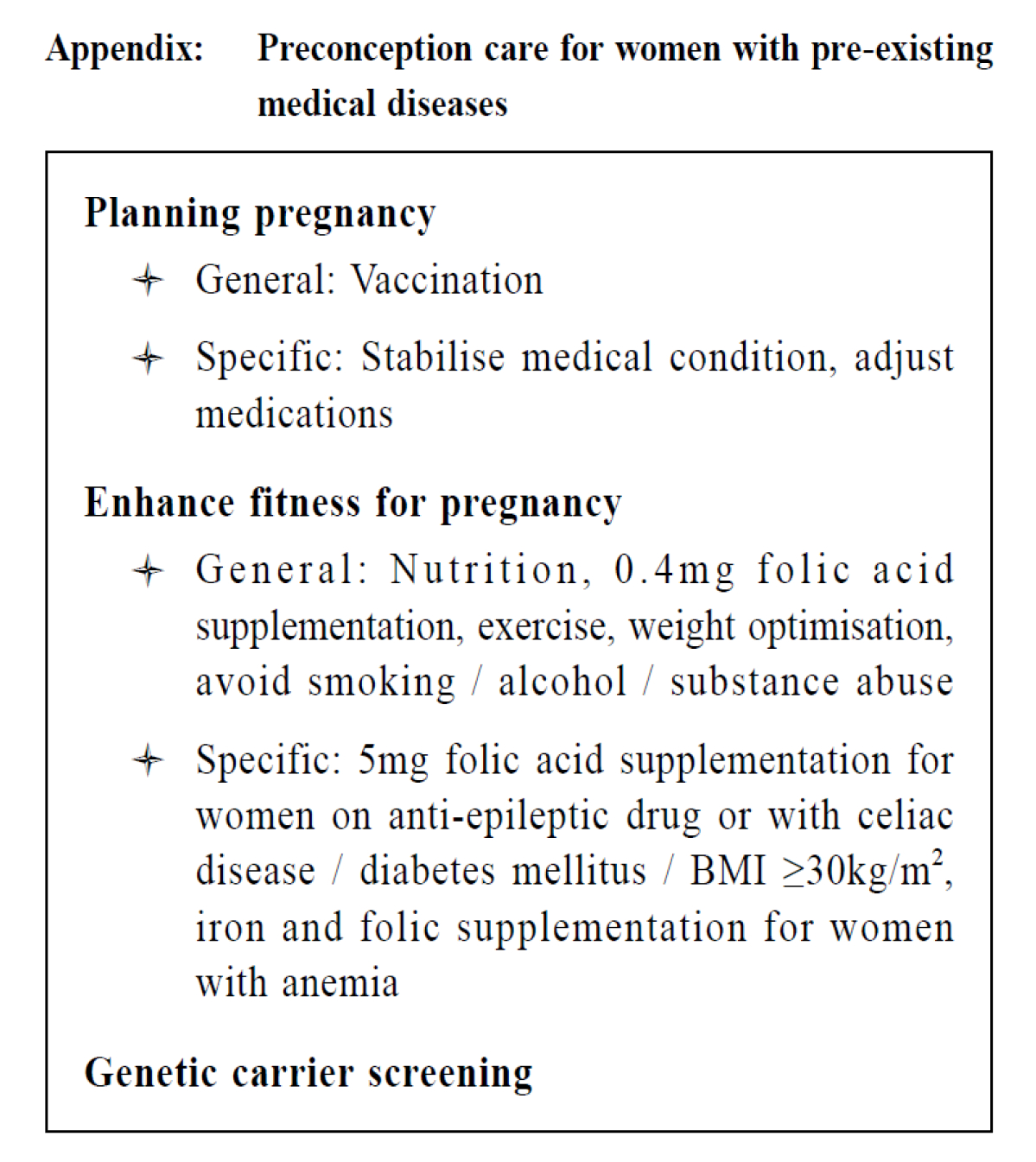
References
Sue ST Lo,
MBBS, MD, FRCOG
Correspondence to:
Dr. Sue ST Lo, The Family Planning Association of Hong Kong, 10/F,
|
|