
|
March 2023,Volume 45, No.1
|
Update Article
|
Conductive hearing loss in childrenWai Tsz Chang 張慧子, Michael CF Tong 唐志輝, Iris HY Ng 伍凱怡 HK Pract 2023;45:12-17
SummaryConductive hearing loss is the most common hearing loss in infant and young children. This can be congenital or acquired. It occurs when pathologies lie within the external ear or the middle ear. Most often conductive hearing loss in children is caused by infection of the external or middle ear. Congenital cholesteatoma is a condition that is easily missed and misdiagnosed as otitis media with effusion. The surgical approach of this disease has largely changed in the current endoscopic era. This educational update article summarises the most current information regarding the causes and treatment options of conductive hearing loss in children.
摘要傳導性聽力損失是嬰幼兒中最常見的聽力損失,可以是先 天性的,也可以是後天性的。外耳或中耳出現病變時會發 生傳導性聽力損失。兒童的傳導性聽力損失往往是由外耳 或中耳感染引起的。先天性膽脂瘤很容易漏診或被誤診為 中耳炎伴滲出。當前是內窺鏡時代,該病的手術方法已大為改變。本篇是最新的教育性文章,總結了有關兒童傳導 性聽力損失的病因和治療方案的最新資訊。IntroductionHearing loss in children reduces their ability of sound detection. Although hearing loss can occur at any age, hearing difficulties at birth or those that develop during infancy and toddlerhood have more serious consequences. The prevalence of permanent significant bilateral hearing loss is approximately 1.33 per 1,000 live births in developed countries.1 Considering the cumulative addition of patients with progressive, acquired or late-onset hearing loss, the prevalence is estimated to be 2.83 per 1,000 children at the primary school age2,3, and a further increase to 3.5 per 1,000 in adolescents.1 Local epidemiological studies in Hong Kong, at the age of 6-7 years old, 5.3% of them suffered from conductive hearing loss, majority suffered from otitis media with effusion.4 Early identification and early intervention is crucial. This does not only apply to bilateral disease, where speech and language development will be affected; single-sided hearing loss should also not be neglected. Previous international studies showed that children with single-sided deafness are prone to a poorer IQ score, worse speech perception especially in noisy environments, poorer localisation, and increased rates of academic failure.5 There are three types of hearing loss: conductive, sensorineural, and mixed hearing loss. Conductive hearing loss occurs in pathology located in the external ear and middle ear while sensorineural hearing loss is caused by abnormalities of the path from the inner ear to the brain. We mainly focus on conductive hearing loss in this article. Causes of conductive hearing loss in childrenConductive hearing loss occurs in pathology located in the external ear and middle ear. It can be congenital or acquired. Congenital conductive hearing loss occurs in kids with microtia or atresia. This can be due to genetic factors or just random. Others can occur in children with ossicular chain abnormalities (due to fixation or absence). A condition known as congenital cholesteatoma occurs congenitally but is usually detected in childhood. Most commonly these children experience acquired conductive hearing loss. These include infection (of the acute otitis media and the otitis externa), and otitis media with effusion (when fluid accumulates in the middle ear from allergies or colds). This hearing loss is usually only temporary; normal hearing commonly resumes once the cold and allergies subside and the Eustachian tube (which connects the middle ear to the throat) drains the remaining fluid into the back of the throat. In some children, perhaps 1 in 10, fluid remains in the middle ear following an ear infection because of problems with the Eustachian tube. Occasionally, we see children with conductive hearing loss having foreign bodies in the external ears, and rarely ossicular chain disruption or tympanic membrane perforation after trauma. Signs and symptoms of hearing loss in babies and childrenIn Hong Kong, the universal newborn hearing screening programme implemented in local birthing hospitals under the Hospital Authority adopts the two-stage Automated Auditory Brainstem Responds (AABR) screening protocol. Neonates are screened within the first 2 to 3 days of life followed by diagnostic Auditory Brainstem Responds (ABR) and a visit to an otorhinolaryngologist. Any presence of hearing loss among these infants, in one or both ears, is confirmed by 3 months of age. However, sometimes newborns who pass the hearing screening can exhibit signs of hearing loss when they get older. Family physicians and paediatricians might detect abnormalities when the child fails to achieve age-appropriate speech and hearing milestones. For example, from birth to four months of age, infants should startle at loud sounds, and respond to one’s voice by smiling or cooing; from four months to nine months of age, infants should turn their head toward familiar sounds and make babbling noises; from 9 to 15 months of age, infants should be able to repeat some simple sounds and understand basic requests; and from 15 to 24 months of age, toddlers should be able to use many simple words, point to familiar objects one names, and follow basic commands. Older children sometimes develop hearing loss in later life. Parents typically complain that their child has difficulty understanding what people are saying, responds inappropriately to questions (misunderstands), and has speech or language delays or problems of articulation. The signs of such hearing loss might be very subtle, such as watching a speaker’s face very intently. In fact, we often encounter delayed diagnosis of many children’s hearing loss because they are very successful lip readers. Diagnosis and hearing tests for childrenWhen a hearing concern is raised clinically, the otorhinolaryngologist will check the child’s external ears. An otoscopic examination will be performed to check the condition of the ear canals, the tympanic membranes and the middle ear. He or she will try to clear up the ear wax or foreign bodies in the external ear canal, if any. The child will then proceed for audiological testing by an audiologist. Apart from the screening and diagnostic hearing tests performed at an early stage of life, which are objective tests, audiologists can test infants as young as 6 months behaviourally. Visual reinforcement audiometry (VRA) can be performed when the infant is able to turn the head toward sound. In this test, a parent will hold their child on their lap while they sit on a chair in the center of the sound booth. The audiologist will play sounds or talk through speakers that are oriented to the left and right of the child. A visual reinforcement toy like a flashing light or dancing bear will be shown to keep their attention. Play audiometry (PA) is applicable to toddlers and preschool children. It is a hearing test that is made into a game for toddlers. The parent or assistant sits on the floor in the booth with the child and trains them to respond to any sound they hear by doing a certain task, like putting a ring onto a rod. Once children are at around 6 to 7 years old, they can usually sit still and raise a hand or push a button in response to speech and tone stimuli in the sound booth, and the pure tone audiometry (PTA) test used for adults can then also be used for them. Treatment optionsDepending on the severity and cause of hearing loss, usually conductive hearing loss is treatable. Treatment varies and can include observation, hearing aids, surgery, and a combination of speech therapy and assistive listening devices. Hearing aidsHearing aids provide immediate hearing assistance by sound amplification. All the hearing aid fitting services for local preschool, primary school, and secondary school children are provided by the Education Bureau (EDB) in Hong Kong free of charge. Hearing aids for conductive hearing loss are indicated for children not suitable for surgery or not willing to undergo surgery. There are special coverings and other accessories to ensure that young children do not remove or misplace their hearing aids. Some other decorative accessories for hearing aids are available commercially. (Photo 1) 
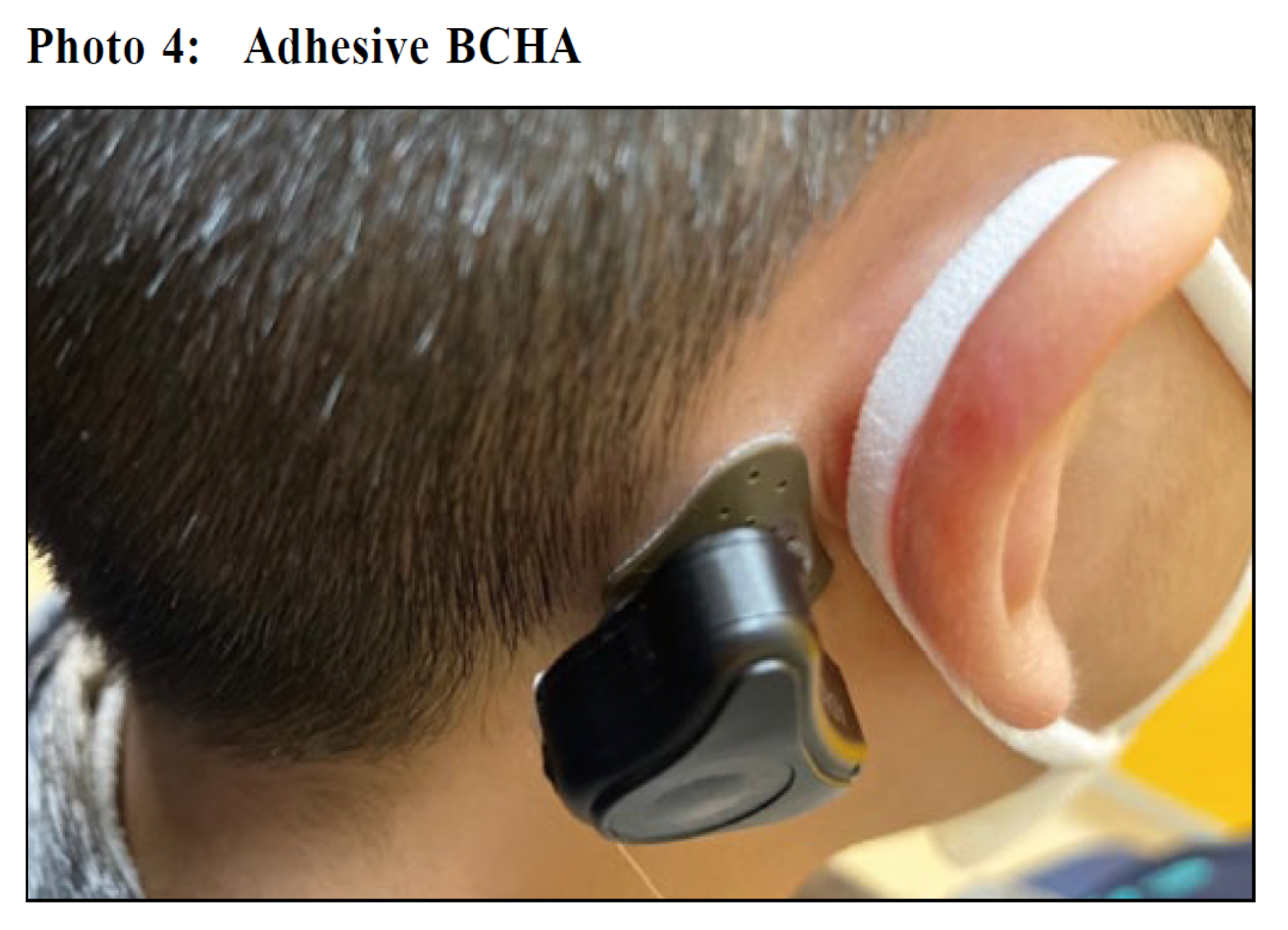
Bone conductive hearing aidsBone conductive hearing aid (BCHA) are special hearing devices that amplify sound via bone conduction. They can be implanted surgically or be fitted non-surgically. Children who may be a better candidate for BCHA typically include those who have severe outer or middle ear malformations, such as microtia or anotia. (Photo 2) They do not have a well formed external ear to anchor conventional hearing aids. In very young children with bilateral microtia, a BCHA headband (Photo 3) is a better option as the skull is too thin for BAHA to be surgically implanted and the kids move so much that the device can easily fall off. Other non-surgical options include adhesive BCHA (Photo 4) to scalp, or a hearing aid worn like a pair of glasses (Photo 5). Conduction is better if the hearing aid rests directly on the skull. Usually after the age of 5 years, the skull bone is thick enough to allow BCHA to be surgically implanted. (Photo 6 and 7). 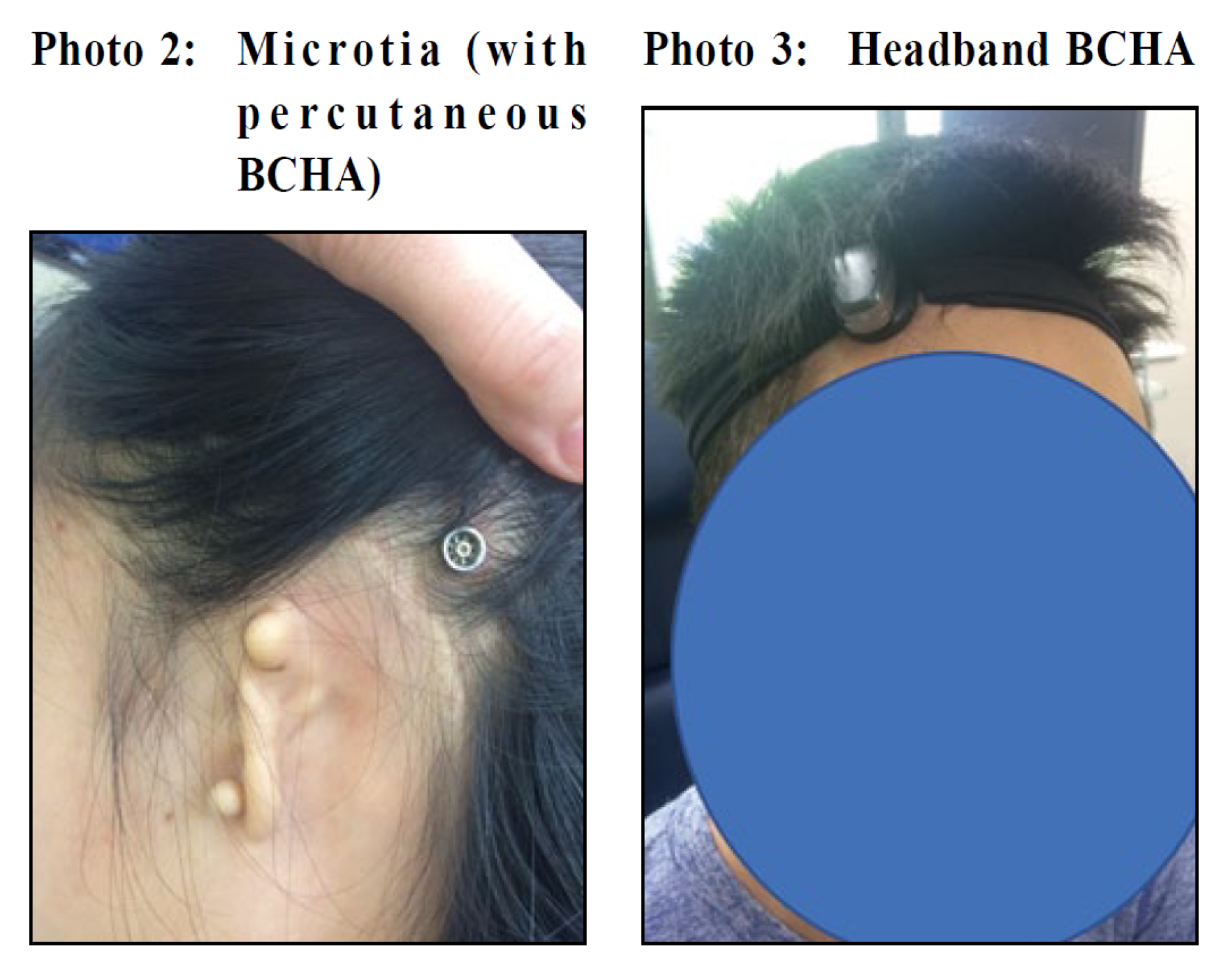


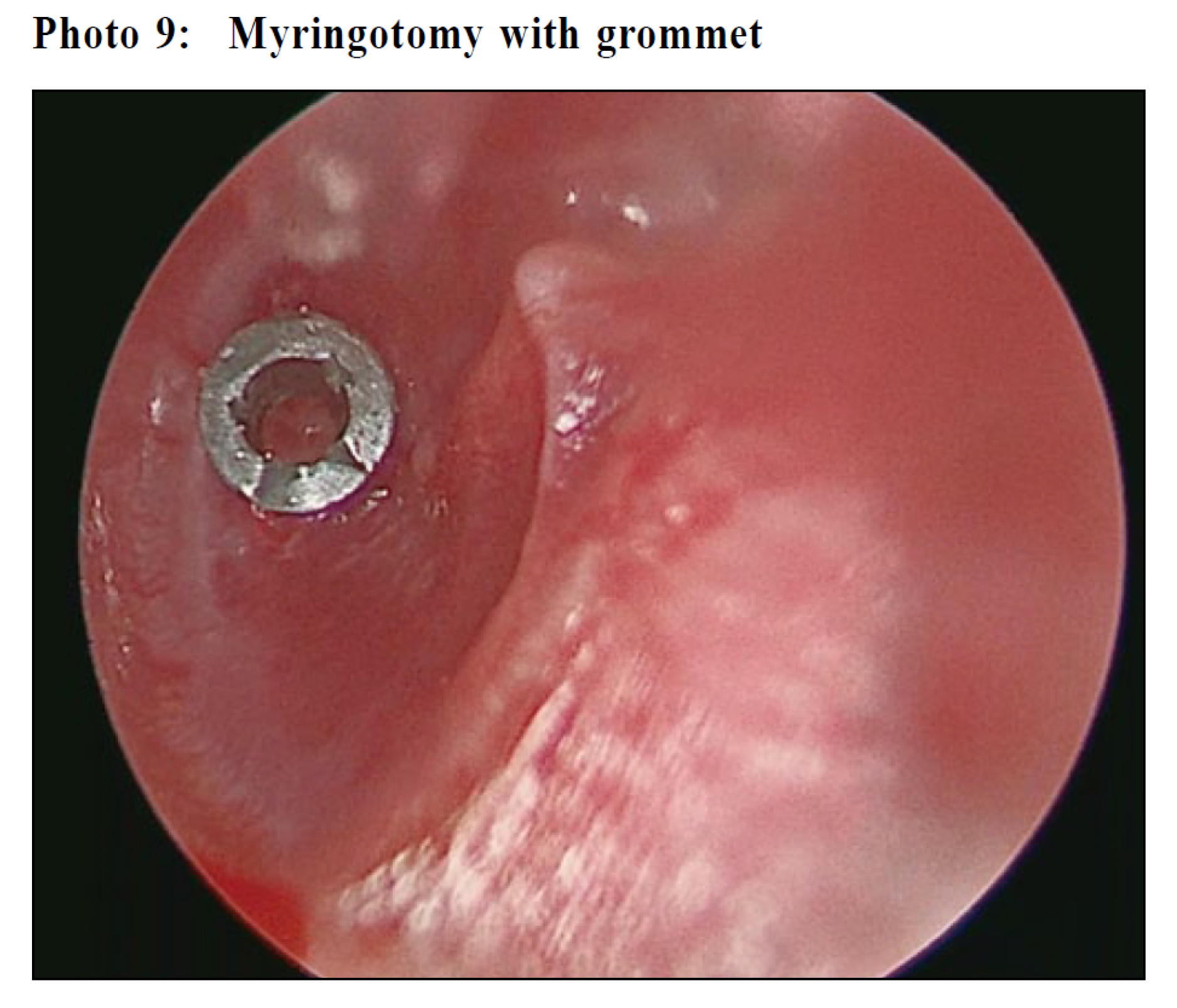
SurgerySurgery is indicated in various disease entities for children with conductive hearing loss. BAHA as mentioned above can be implanted surgically. Other surgical treatments for children are indicated below: Myringotomy and grommet insertionMyringotomy and grommet insertion (M&G) is the most commonly performed otology operation in children, usually indicated for middle ear effusion (Photo 8). Small amounts of fluid are normally produced in the middle ear and usually drains out of the ear through the eustachian tube. A middle ear effusion occurs when fluid builds up in the middle ear, which can cause problems in hearing. This happens most often after an ear infection (otitis media) but can also happen without a preceding infection. It is very common, especially in children aged 2 to 7.4 Approximately 90% of children will have fluid build-up in the ear at least once before they begin school, according to the American Academy of Family Physicians. This condition most often clears up on its own within 4 to 6 weeks.6 Antibiotics are usually not needed. About 10% of children will still have fluid in the ear 3 months after the infection clears up. If the condition persists for more than 3 months, M&G will be considered. This procedure is done under general anesthesia.7 An ENT surgeon places a small drainage tube through a small incision in the eardrum to help fluid drain out. Hearing should improve immediately after the operation. (Photo 9) 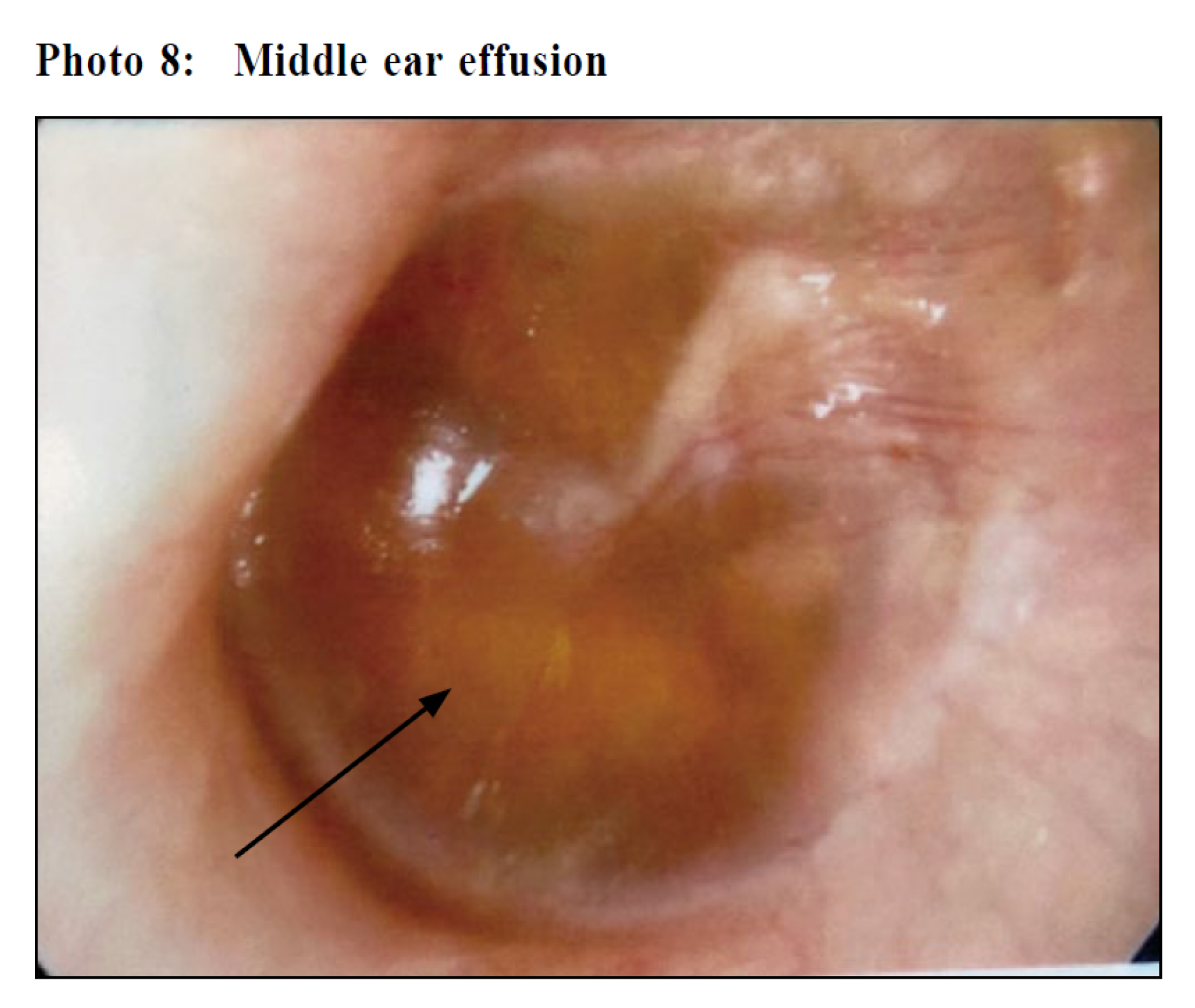
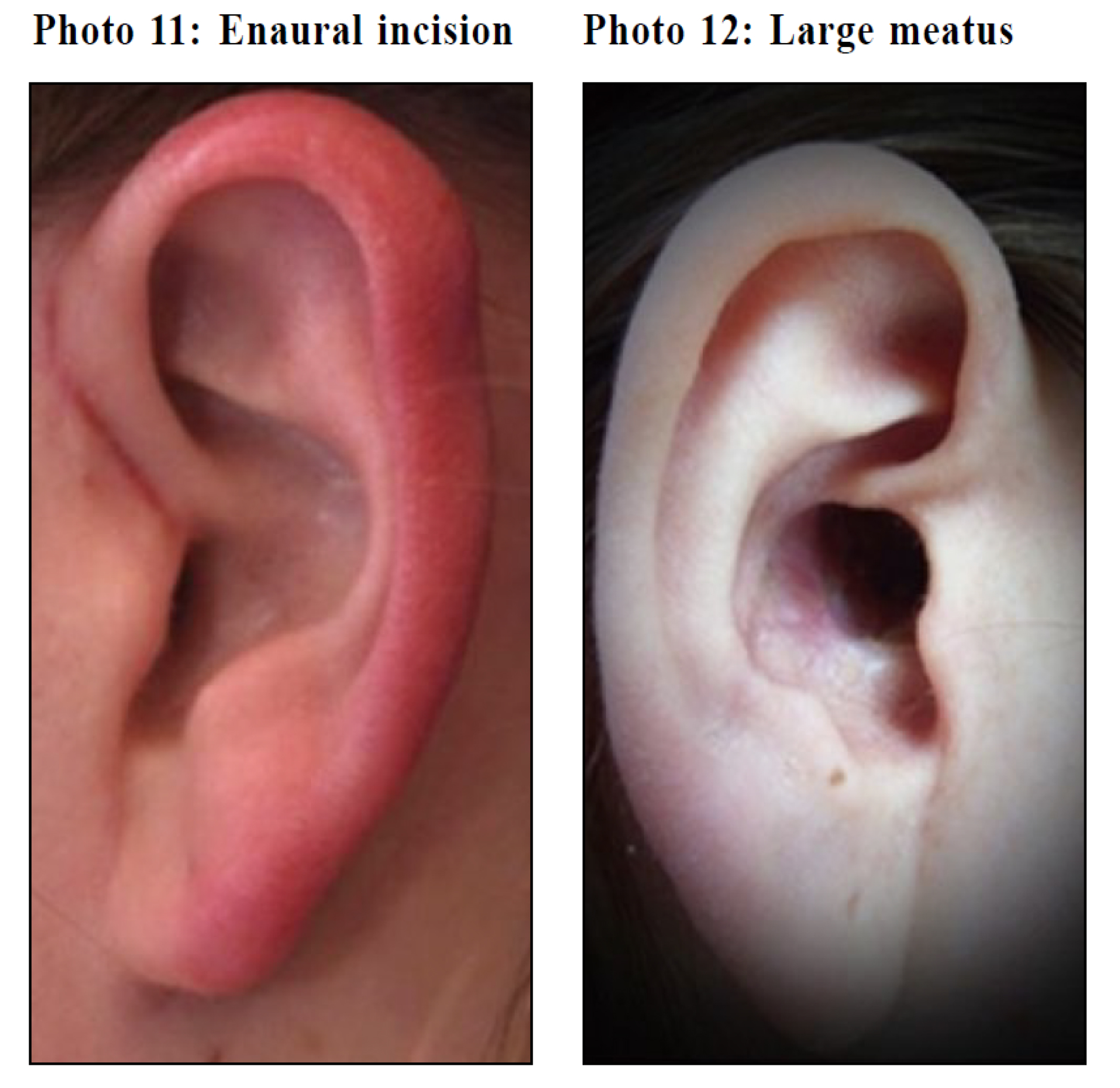
MastoidectomyMastoidectomy is indicated in acute scenarios including acute mastoiditis. Usually the child is very ill and presents to the emergency unit with sepsis with fever and postauricular erythema and swelling. More chronic or subtle middle ear disease presenting as unilateral (or sometimes bilateral) hearing loss that eventually requires mastoidectomy would be congenital cholesteatoma. Congenital cholesteatoma is defined as a whitish mass behind an intact tympanic membrane in the middle ear, mastoid, or even petrous apex, which pathology shows to be keratinising squamous epithelium. It is easily missed and sometimes misdiagnosed as middle ear effusion, therefore making the actual diagnosis rather late. However, it can cause significant problems because of the erosive and expansile properties of congenital cholesteatoma. This can result in the destruction of the ossicles and skull base. They often become infected and can result in both conductive or even sensorineural hearing loss, facial nerve palsy, meningitis, dizziness, and chronically draining ears. Treatment almost always consists of surgical removal. Traditionally, ear surgery will be performed using the surgical microscope via a post-auricular incision (Photo 10) or enaural incision (Photo 11) and meatoplasty resulting in a large external ear opening (Photo 12). In recent years, with the development of endoscopic ear surgery, congenital cholesteatoma surgery can be performed without an external wound (Photo 13) and with better visualisation of disease and better disease clearance. Patients can be discharged on the same day without heavy ear packing or head-bandage. Tympanoplasty and OssiculoplastyTympanoplasty is performed to repair the tympanic membrane to help restore hearing and prevent infection. This procedure may also involve reconstruction of the ossicles (ossiculoplasty) if needed. Both the tympanic membranes and ossicles need to function well together for normal hearing. This procedure is usually not performed in children under four years of age as their eustachian tubes do not yet function well and otitis media may occur. Abnormalities of the ear drum and middle ear bones can occur through previous M&G, ear trauma such as through the use of cotton buds, otitis media, congenital deformities, or erosion by cholesteatoma. Therefore, these procedures are sometimes performed in combination with mastoidectomy in indicated cases. During the tympanoplasty, the eardrum is lifted up and the graft (usually an autograft from the temporalis fascia or the perichondrium) is slipped behind the eardrum. If problems with the ossicles are seen, an ossiculoplasty can be performed with an autograft (usually fashioned ossicles) or an allograft (usually a titanium prosthesis) in the same operation. A paediatric tympanoplasty or ossiculoplasty can usually be performed completely through a small front of ear incision (enaural incision) (Photo 11). However, many children have small ear canals that are difficult to work through, or the perforation is very large and cannot be completely seen through the ear canal. In these cases, a larger incision is made behind the ear (a postauricular incision) (Photo10) in order to improve the visualisation. In the current era of endoscopic ear surgery, these incisions can usually be completely avoided. (Photo 13). 

Speech therapyChildren who have had hearing loss that has affected their speech might need speech-language therapy after getting hearing aids or surgery in order to help them catch up after speech delays. Such therapy requires specialised paediatric speech therapists to proceed. 
Assistive listening devicesMany hearing aid manufacturing companies offer assistive listening devices such as FM systems that are discreet and work well in a classroom situation in conjunction with the child's hearing aid or implants. (Photo 14) FM technology helps overcome the poor acoustics of classroom settings or other venues with lots of background noise. The teacher wears or has a discreet microphone in front of him or her that transmits his or her voice directly to the child's hearing devices. 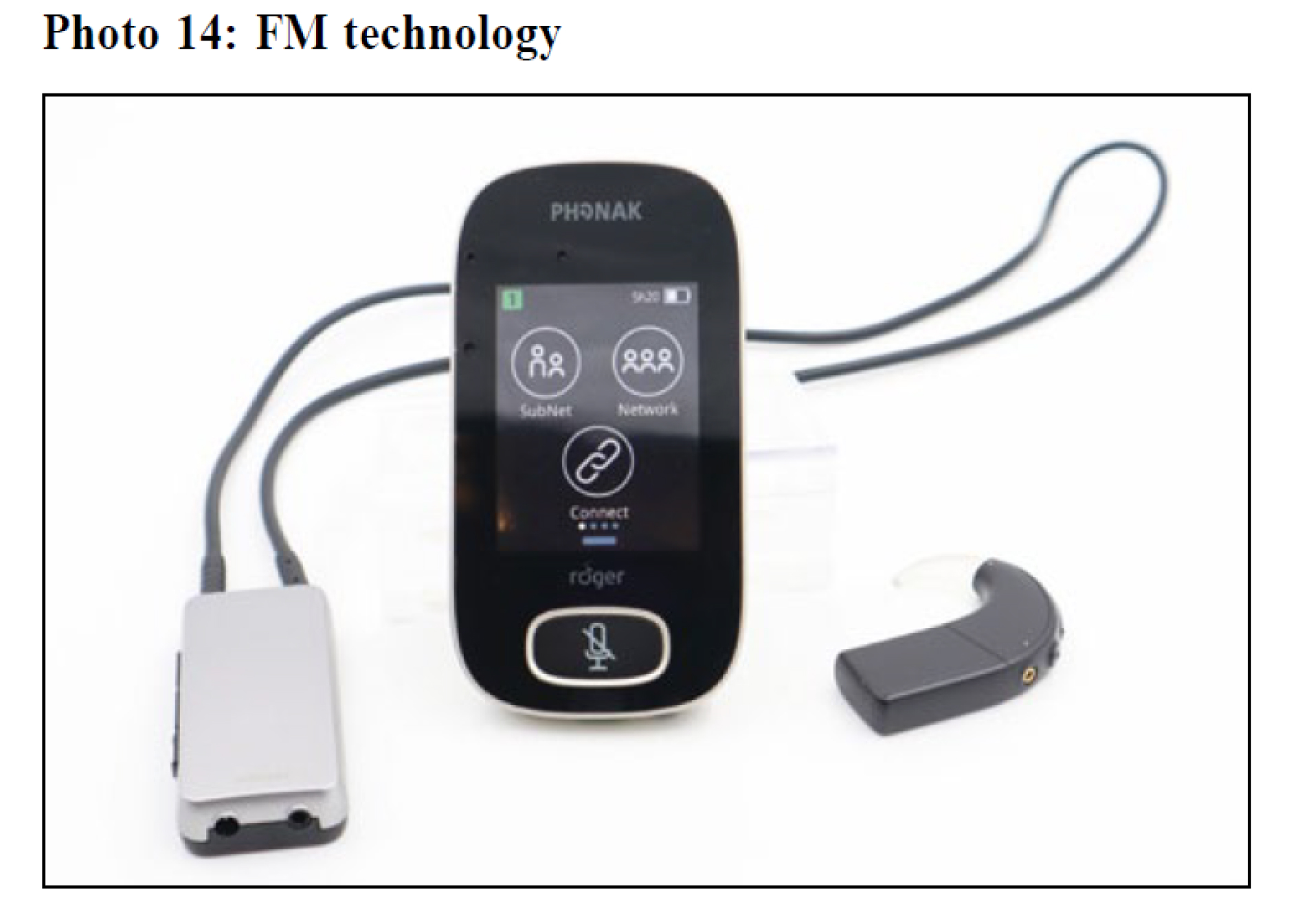
Assessment and management of conductive hearing loss in primary careHearing loss in children is very common and are clinically significant. Any delay in diagnosis might affect the speech and language development and surgical outcome of the kids. If primary physicians encounter any infants whose hearing has not been previously screened, their parents should be advice to have them attend screening audiometric assessments. In children aged 2-7, the most common cause of conductive hearing loss is otitis media with effusion. High index of suspicion shall be given to kids with upper respiratory tract infection. Parental suspicion of hearing loss in children is not very reliable. The positive predicted value was 82% in local studies9 vs 70% in the Netherlands10. So do not hesitate to have a check on a tympanogram or a screening audiometry if you encountered any kid with suspected hearing loss. Early referral to Otorhinolaryngologists for proper diagnosis and early treatment is required. ConclusionConductive hearing loss is a very common condition in children and the disease spectrum can be varied. Early identification is needed, and becomes possible when parents and teachers can pick up on trivial signs and seek medical advice early. Correct diagnosis can direct precise treatment. Endoscopic ear surgery helps to minimise the wound and increases precision. A short operating time and hospital stay, and early recovery, can be achieved References
Wai Tsz Chang,
FRCSEd(ORL), FHKCORL, FHKAM, MScEPB
Michael CF Tong,
MD, FRCS, FHKCORL, FHKAM
Iris HY Ng,
PhD, MSc (Audiology)
Correspondence to: Dr. Wai Tsz Chang, 6/F Lui Che Woo Clinical Science Building,
|
|