
|
December 2024,Volume 46, No.4
|
Plenary of Hong Kong Primary Care Conference 2024
|
Medical social collaborationChing-choi Lam 林正財 HK Pract 2024;46:100-105 My topic today is medical social collaboration which I believe is one of the “connections” that this conference is talking about. Apparently medical social collaboration is a very trendy and sexy word. It has been talked about in Hong Kong for nearly 20 years but to the government this is a pretty new term. I still remember when we were going to restructure and rebuild our whole preventive primary care system, I talked to the chief executive at the time, that we must put this phrase “medical social collaboration” into the Government Policy Address. Our policy address is a very important document for the whole running of our government. It was instilled not once but 4 times into her Policy Address: So, I hope to share some the thinking behind this. While I am sitting in a number of committees, one of them is the Carbon Neutrality and Sustainable Development Committee. This sustainability is just as Dr. Libby Lee has mentioned. Our health care system is one of the sustainable developments we are looking at. While we are talking about sustainability, most of the time we are talking about supply and demand. How can we keep this balance so as to make that particular system sustainable. This demand is growing quite steeply and accurately in Hong Kong. Part of this is because Hong Kong is a “super- aged society”. Not only an “aged” society but a “super- aged” society according to WHO. Along with this aging, the number of chronic diseases is increasing, so according to the Hospital Authority, represented here by Mr. Henry Fan, its chairman, the number of chronic disease sufferers will rise to 30,000 or 40,000. As we can see, we have a huge burden. While we are talking about health care sustainability particularly on the financial side and obviously, we have the human resources side, our public health expenditure is increasing steeply as you can see the distribution in Figure 2. Figure 1 
Source:https://www.primaryhealthcare.gov.hk/bp/cms-assets/Primary_Healthcare_Blueprint_Saddle_Stitch_Eng_a1acc40d18.pdf Figure 2 Health System Sustainability 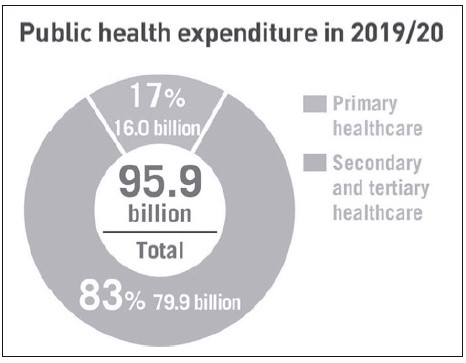
Source: Domestic Health Accounts 2019/20 Most of the expenses were on curative care especially in the form of tertiary institutes in Hong Kong, whereas the percentage is actually shrinking for the primary care especially on the preventive care. So, while we spend more and more on curative care but despite the amount of money given to the Hospital Authority, the percentage put into preventive care is getting smaller and smaller with this total amount being 90% of our total government expenditure. So as fair as sustainability goes, we must look at this unhealthy situation. This is a very famous pyramid. So, in Hong Kong as I have already mentioned, much of our expenses were put into our tertiary health care and unfortunately, well I can’t say unfortunately, actually it is fortunate that 70% of the Primary care is provided by the Private sector. While we are talking about preventive primary care, it is unfortunate, because most of the Hong Kong citizens pay their primary care out of their own pocket or via their insurance. Our insurance product is not very conclusive to preventive care either. So, people tend not to pay for prevention. Hence the government, that is the last term of the last government took up the very important task of providing and restructuring the whole preventive primary care system, which is very reasonable especially according to Professor Doris Young here. This was forecasted, planned and advised for the government to implement many many years ago. So finally, as I have previously mentioned, we have the Primary Healthcare Blueprint just 2 years ago which I would say is a very important document shaping our primary care system. I had the privilege to be involved in developing this Blueprint. As mentioned by Dr. Libby Lee, there are 2 elements in our Blueprint, one is how do we vertically integrate our tertiary system back into our primary care system. Figure 3 Paradigm Shift Needed in Healthcare System 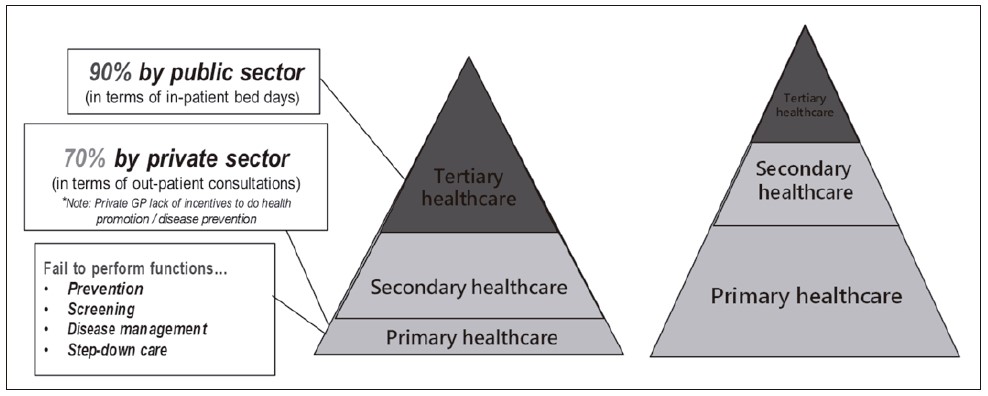
Source: Food and Health Bureau, Health Care Reform Consultation Document Appendix B Hong Kong’s Current Healthcare System (2008) Figure 4 
Source: https://www.primaryhealthcare.gov.hk/bp/cms-assets/Primary_Healthcare_Blueprint_Saddle_Stitch_Eng_a1acc40d18.pdf In Hong Kong, we are different from the UK NHS (National Health Services) or any other healthcare system in the world. We basically don’t have gatekeeping and we don’t have a well-articulated “step down” system. So, all patient care will finally stream into our hospitals, which as medical professionals we all know is unhealthy and not sustainable. So, with vertical integration, we aim to build a gate-keeping system from this status quo into a healthy financing system in Hong Kong. We know that this is not going to be easy as we do not have the financial tool on hand and it is literally very difficult to direct our patient flow. However, if we are not going to reform our financings system radically then we must find some way to integrate and guide the patient in their pathway. Also, in the vertical integration we will build a step-down system with as mentioned the District Health Centre (DHC) in place. Today we are not talking about this vertical integration, we are talking about the horizontal one which is the medical social collaboration. I must say that this word, social is not only talking about social services, we will broaden it in its social context and include a world bank definition on social capital. Meaning how do we use the social capital to take care of our population’s health. Within our community we have the DHC the public health services, the general outpatient clinics and our “traditional” social welfare services. We actually have a lot of community initiatives working together to make our population healthy. This includes the healthy city initiative which is the WHO initiative and have been implemented throughout all Hong Kong’s 18 districts. There are also a lot of community organisations working directly and indirectly involving health care including the 關愛隊(Care Teams) which has been established in Hong Kong. So, we can lobby everyone together. Togetherness is also a key word, so much so that we can build our community conductively to the population health. This is the objective of the whole thing. The established chronic disease co-care pilot scheme is a very important initiative. We are building the DHC and the DHC Express, which is still in its infancy stage. I am a paediatrician, so I know that it takes time for a young child to grow and likewise for a system to grow, it will take an even longer time. So, ladies and gentlemen and especially our medical doctors, you may have a lot of expectation from this system. You may even complain that the system is not helping you do your job well at this stage in time. Please allow room for it to grow and mature. It takes time, but I would say that it is heading in the right direction. Let them have some time to grow and mature, to build trust and build momentum. This pilot scheme is one of the important tools to build the “Family Doctor for All” ideology. Figure 5 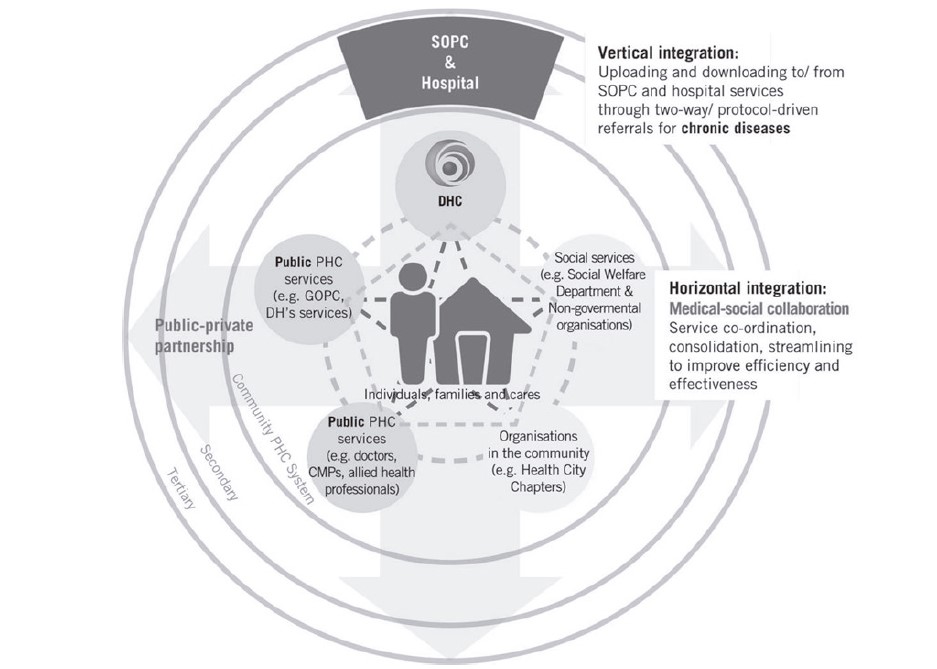
Source: https://www.primaryhealthcare.gov.hk/bp/cms-assets/Primary_Healthcare_Blueprint_Saddle_Stitch_Eng_a1acc40d18.pdf As I have mentioned, 70% of the curative care is being delivered by our family physicians and the general practitioner. Because of this financial system, Hong Kong people like to shop around. This basically is consumer behaviour. Only 23% of our citizens actually do have a family physician. But with this scheme they must choose their own family doctor. For the first time we have the establishment of the electronic personal health records, which is called “e-health” and in the future, we will upgrade this to the “e-health plus”. Our citizens will have their name on their individualised e-health record stating that “Dr Samuel is my family doctor”. I would say that this is an extremely important move made by the government to recognise the family doctor in Hong Kong. This e-health system is being established by our government but our legislative council members complained that we are putting too much money into it. To me, it is money well spent. So please for doctors, do join this co -care programme. This is one way, one important way to build the “Family Doctor” concept in Hong Kong. You may complaint about the details of the system but this is the big picture of how we will be establishing “the Family Doctor system” in Hong Kong. This scheme is going in the right direction. I would like to have more family doctors joining and then more and more citizens will join. The results are quite promising, in a way that a lot of our citizens are actually having undiagnosed hypertension, undiagnosed diabetes, but even more importantly, we identify a lot of citizens with risk factors for pre-diabetes. That means with good community support, they can take care of their own health much better. So, this is one of urges for us to build this medical social collaboration. As I have mentioned before, the role of the family doctor is very important in this Blueprint, I don’t want to over emphasis it today. From the prospective of the general citizen, the family doctors are the major primary care service provider providing comprehensive, personcentred, continuous, preventive and co-ordinated care for them and their loved ones. They have a crucial role in supporting the person continuously in the prevention and self-management of disease. As we try to build medical social collaboration, we find that the gap between the Family doctor and the medical social services is still quite significant. So, our rule is to narrow the gap. The government as I have mentioned have stepped up and for the first time in the government document, medical social collaboration is stated as a policy objective. We can image that there is a huge gorge dividing the medical and social sectors. In order to cross over and connect the two, a strong bridge needs to be build. So, I hope that we can all build this bridge together. While we are promoting population health we must work up-stream. All or shall I say most doctors are working in the wells downstream, the whole Hospital Authority is way downstream. They can hardly influence anything or affect any that is happening upstream. There are a lot of upstream reasons for a person to become sick, unhealthy and/or to suffer from a chronic disease, I think we all know this. As the chairman of the Council for Carbon Neutrality and Sustainable Development, I must say that we should add another factor affecting the health of our citizen. This is the hot weather. The weather climate affect disease patterns and hence our health. Traditionally a medical doctor has nothing to do with any of these factors. We have to build effective collaborations so that we can have leverage on all our social workers, this does not only mean social welfare workers but workers in the community. For want of a better term, it is best to say community workers to handle all these upstream issues. I know that this is not easy, we must build trust among different groups of people. Especially we doctors tend to work within 4 floors, either in a clinic or a hospital. So, we must learn the language and understand our partner and narrow the knowledge gap on disease management. One good thing the government is doing via the Primary Healthcare Commission, is to build protocols so that everybody is working on the same platform. So, record sharing and all this stuff we need to do, but as Dr. Tony Ko always says, he being a Geriatrician and one who knows everything about medical social collaboration. He says trust is the number one thing to building collaboration, not governance, not law and order, not regulations but trust. We cannot force collaboration by bringing in more regulators. We can only build collaboration by trust. We must step up and understand each other well. The “Revolving door syndrome” is one of the known syndromes with our system and one which is making our community more and more expensive. Because our community is not adequate, the collaboration is inadequate or not strong enough to handle or to support our patients who have been discharged back to the community. So, they will very easily go back into hospital. End of life care is a typical example of this syndrome. For each individual who is going into the last stage of their lives, they might need 3 to 4 admissions into the Accident and Emergency departments or even into the intensive care unit or medical ward before they can pass away peacefully. Our government is determined with Dr. Libby Lee’s support, to reform our law We are changing our ordinance and having our advance medical directive so that people can really choose where they want to die. Dying in a place of their choice. For the time being, 90% of our deaths happen in the hospital, which is not one of the highest but THE highest in the world. That means we are not providing choices for the individual person and their families but now we are going to provide the possibility of a choice. To provide this, we must collaborate and require more family physicians and general practitioners who are willing to do home visits. “Home” meaning the nursing home or the domestic home. We need more training so that we can do this. I know that pricing is one of the hurdles. I advocated to the government on how we can subsidise a little bit so that doctors can do home visits better. We must rely on the social care system to take care of the meals and the nursing and everything so that the individuals are willing to die in a place apart from the hospital. In all the studies done as well as the one done in our locality, the end-of-life care programme is and does save money for the hospital system. We save 3 to 4 accident and emergency admissions and 1 to 2 intensive care unit admissions as most of these are not necessary for that individual. So, I would say that medical social collaboration is one of the keys to making our healthcare system sustainable. Figure 6 
After when I was appointed as the chairman of the Advisory Committee on Mental Health, I found that there were a lot of opportunities and challenges too. A lot of things can be handled with better collaboration. Since today the topic is not on mental health, so I will not go into details, but I can see there are a lot of opportunities for collaboration even for our psychiatrist to go online to help those hidden troubled youngsters who otherwise will not go to see any psychiatrist or seek help from any kind of institutes before they commit suicide. So, we must collaborate in a very creative way. On the social side, we have a good system which we are using. The youngsters can approach us via Instagram (IG), by Messenger, by Whatsapp, by whatever means. I am planning to set up a surveillance system in a virtual world, via social media to actively detect and search for those hidden troubled youngsters. Our referral rate for all young persons who fail to see a psychiatrist is from 70% to up to 90%. We cannot just rely on our traditional medical system to handle this for the present “new” generation and less so even for our newer generation where AI is coming too. I am urging all of you to think more creatively while we are doing more collaboration. As I have mentioned before, there exist 2 sectors each having 2 separate languages even their emphasis is different. Our medical community is very good at practicing evidence-based medicine, which is good but our partner might not know or understand what evidence-based medicine is and/or how it operates. How can we build trust so that our methods of doing things are aligned with each other? It takes time. If we are to trust, we can reconcile our cultures. Training enhancement, as I have said, are needed to revamp our whole training culture including our medical training. How will our medical student know what is happening in their community right now? I urge our esteemed college to do more training so that our family physicians should have experience in providing social and community care better. I will be attending the British society for Lifestyle Medicine conference in September. I believe that lifestyle medicine maybe a good platform for all professionals coming together to make sure that all our preventive primary care system can build on how to promote a better lifestyle. Finally, Organic collaboration, what do I mean by this is? I mean that we should not be working for cooperation, we should be working for collaboration. This means that in our medical system we must have a social element, and in our social system we must have a medical element. Just like in China, for long term care they have a very good system called 醫養結合 (Integrated medical and nursing care) which is where they are putting the medical world into their long-term care system. We have a little bit of this already. We will be building a mega nursing home in Hong Kong soon but unfortunately; we are not yet at the stage that we can collaborate in an organic and realistic manner. This is my hope and sincere wish that we will be having more and more talk on medical social collaboration and more importantly more and more action. * This article is based on a plenary lecture given by Dr. Lam Ching Choi at the Hong Kong Primary Care Conference 2024 of the Hong Kong College of Family Physicians.
Ching-choi Lam,
SBS, JP MBBS(HK), FHKAM(Paed), FHKCPaed, FHKCCM, MRCP(UK), DCH(Ireland)
|
|