
|
December 2024,Volume 46, No.4
|
Plenary of Hong Kong Primary Care Conference 2024
|
Family medicine: connecting the right services at the right time to the right personCindy LK Lam 林露娟 HK Pract 2024;46:106-110
Introduction“Our value to medicine lies in the differences… Eventually… the academic mainstream will become more like us than vice versa…” Professor Ian R. McWhinney, 1926-2012.1 Family medicine distinguishes itself from other specialties in that it specialises in the person, instead of a particular condition, organ system or group of people. Our main differences of system thinking, context sensitivity, continuity of care and adaptability to changes make family medicine the best fit for the purpose of the reformed primary care envisioned in the Government Primary Healthcare Blueprint.2 This paper will discuss the new norm of primary care; the need of a transition from multidisciplinary to integrated medical-social model for primary care; and the strengths, weaknesses, opportunities and threats (SWOT) of family medicine in serving its new primary care roles.
The New Norm of Primary CareThe success of rapid advances in health science has lengthened life-expectancy by delaying death, but many diseases remain incurable. The result is an ageing population with many people living with an increasing number of chronic diseases and years of ill-health. This is the phenomenon of “the Failures of Success” described by Ernest M Gruenberg.3 Furthermore, new health intervention technologies are increasing exponentially with the promise of more and more state-of-the-art but very expensive treatments. Easy access to health information, which is often unregulated, has created high expectations from the public. The end result is an excessive demand for more and better care that puts the sustainability of healthcare systems in crisis all over the world, and particularly in rapidly aging populations such that of Hong Kong. A shift of more healthcare from the hospital to primary care is the only solution to contain costs and to assure better equity and quality of care.2 The landscape of primary care has changed from episodic treatments of self-limiting and minor illnesses to the long-term care of people with multimorbidity and complex bio-psychosocial problems. The new primary care needs to personalise care with prioritisation and sometimes trade-offs among multiple medical and social needs. To be effective, primary care must address the social determinants of health4 in the care of patients with chronic diseases and mental health problems that often co-exist. Primary care is expected to provide more care but at lower costs in the mission of value-added services. To serve the purpose, primary care needs to redefine its structure, process and outcomes. (Figure 1) It needs a structure with an open system that can connect medical, social and community services to the patients and their families. An open system can adapt to the changing needs of the patient, healthcare system and the community. The traditional primary care team of doctors and nurses must expand to become a transdisciplinary team that includes physiotherapists, occupational therapists, dieticians, pharmacists, social workers, clinical psychologists, community volunteer workers and others, who can be readily accessible by the patient when a need arises. The team members need not work under the same roof, but they must have effective coordination and continuity of care. Pooling resources from different healthcare sectors, social services, NGO and other community partners can create synergy and add value to each individual service. In addition to evidence-based treatments of individual illnesses, the process of primary care should also include patient enablement and empowerment so that patients become wiser in making decisions affecting their lives and health. An integrated biopsychosocial-behavioural approach to care is often required in the management of chronic diseases and mental health problems. Figure 1: The new norm of primary care 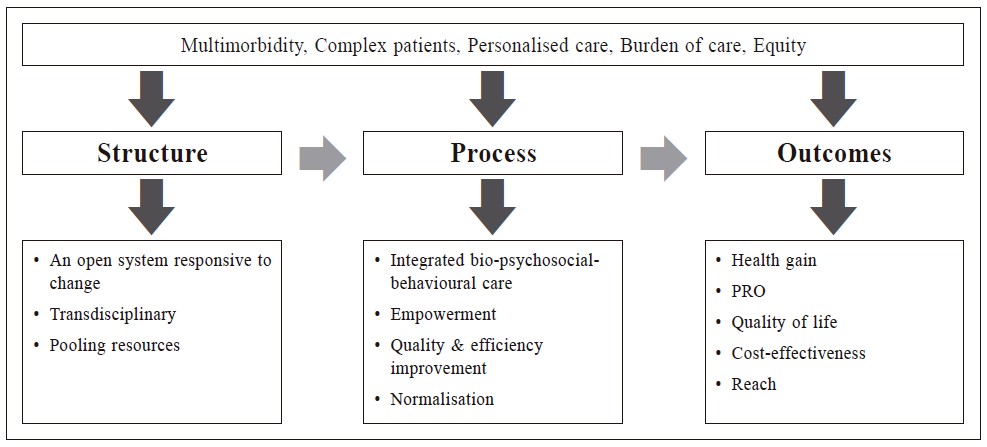
Social prescribing is becoming part of routine primary healthcare in the United Kingdom and some other countries including Mainland China and Singapore5-7, although it is a still a relatively new concept in Hong Kong. The territory-wide district health centre/express establishment is an ideal structure to facilitate social prescribing. The outcomes of primary care should be measured not only by the traditional biological indicators of diseases, but also by the overall health gain, patientreported outcomes (PRO) in terms of quality of life, enablement and satisfaction. The cost-effectiveness of primary care should be measured in the context of the overall service provider and societal perspective, in that the incremental investment to enhance primary care is balanced against the savings in total healthcare and social costs. A unique strength of primary care is its scaling effect; therefore, the reach of good practice is an important outcome indicator of quality of care.
From Multidisciplinary to Integrated CareMultimorbidity with chronic diseases and mental health problems is a great burden to the person, the family and the healthcare system. The main stay of chronic disease care, from prevention to rehabilitation, is self-care with modifications in behaviour and the social environment. To be effective, we need an integration of medical-social-behavioural care that addresses both the biological. emotional and social determinants of health. While the traditional multidisciplinary care model operates by referral, in which each professional provides its service within its boundary, the integrative care model brings different professionals to work together with shared objectives, services and resources without rigid disciplinary boundaries. This allows a dynamic integration of medical, social and behavioural interventions for an individual person, and it provides comprehensive care from improvement in health literacy, enablement and empowerment of life-style modification, self-care and appropriate use of services and to coping with illnesses. An example of medical-social integrated care is the KGKF-HKU Health Empowerment Programme (HEP) that has demonstrated the feasibility, sustainability and effectiveness in improving health for low-income families.8 The HEP integrated the services from six medical disciplines and over 10 NGO and community partners to reach the hard-to-reach low-income families, to engage them in regular health assessment and empowerment activities, and to facilitate their access to the appropriate medical and social services. A comparative evaluation between adult participants of the HEP and adults from comparable low-income families who had not participated in the HEP showed significantly greater increase in self-care enablement and mental health (Table 1)9 and greater improvement in ideal cardiovascular health (Table 2)10 in the HEP group after a mean follow up of 5 to 6 years. A comparison of children from families who had participated in the HEP with those from comparable low-income families who had not participated in the HEP showed significantly greater reduction in behavioural difficulties and a significantly greater improvement in prosocial behaviour and psychosocial health-related quality of life in the HEP group after a mean follow up of 54-56 months (Table 3). Working together with local NGO, the HEP was able to engage asymptomatic adults and children in regular health assessments to identify and treat health risks, e.g., overweight and obesity, hyperlipidaemia and depressive symptoms, and diseases, e.g., pre-diabetes mellitus, diabetes mellitus and hypertension, early. The HEP also motivated low-income families to be more health conscious and empowered them to take action to improve their health. Apart from NGO, the project also connected many local resources including space, service providers and volunteer workers to the people in need. Table 1: Changes in self-care enablement and health status in adults from families participating in HEP and those from comparable low-income families 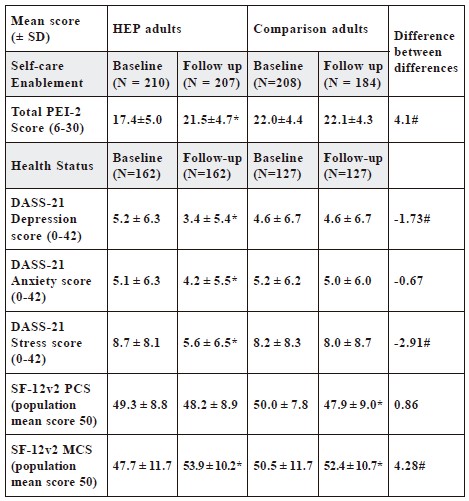
HEP: Health Empowerment Programme; SD: standard deviation; PEI-2: Patient
Enablement Instrument-version 2; DASS: Depression, Anxiety and Stress Scale; SF-
12v2: Short-form 12 Health Survey-version 2; PCS: Physical component summary
scale; MCS: Mental component summary scale.
Table 2: Changes in ideal cardiovascular health in adults from families participating in HEP and those from comparable low-income families 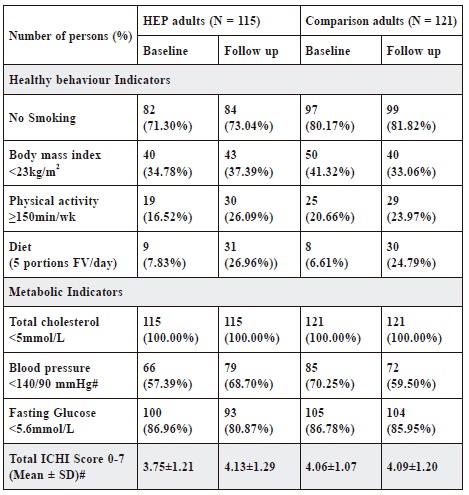
HEP: Health Empowerment Programme; SD: standard deviation; ICHI: Ideal
cardiovascular health
Table 3: Changes in behaviour and health-related quality of life in children from families participating in HEP and those from comparable low-income families 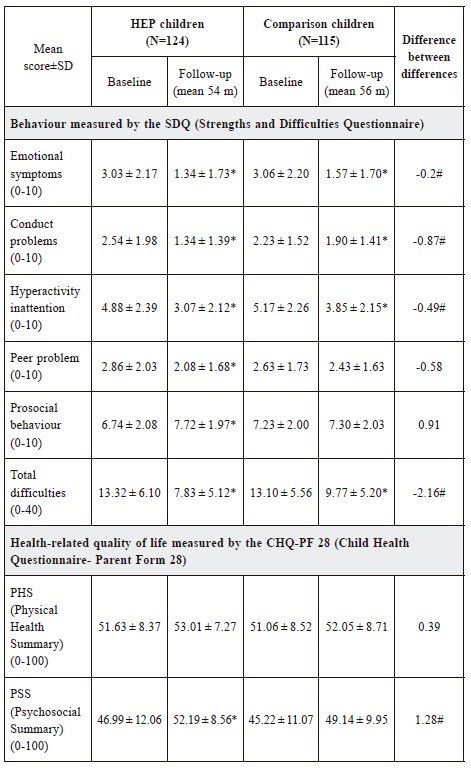
HEP: Health Empowerment Programme; SD: standard deviation
Family Medicine: Connecting Services to the Person“…… It is more important to know what sort of person has the disease than what sort of disease the person has….” Hippocrates 460-357 B.C. The core value of family medicine is the commitment to the person1 with the goal of enabling and empowering the person to stay healthy, recover from illnesses, lessen discomfort, and reduce suffering. The range of services available to primary care is wide and will continue to increase to meet its new roles, but more is not always better. Different individuals may benefit from different services, and a particular person may require different services at different times. A mismatch between the persons and services is ineffective, burdensome and wasteful. Family medicine is the best fit for the purpose of the new primary care to ensure the right services are connected to the right person at the right time. There are many strengths and opportunities for family medicine to take up the leadership role in the new era of primary care, but there are also some weaknesses and threats (Figure 2). The most notable strengths of family medicine are the competencies in person-centred care, system thinking, bio-psycho-social-behavioural integration and cost-effective use of resources, and the skills in interpersonal and communication skills, multidisciplinary care co-ordination, multi-tasking and team leadership. The major weakness that hinders family medicine’s progress is its identity and role confusion.11 There is still uncertainty on whether the discipline should be called family medicine or general practice, and there is no consensus on who can qualify to be a family doctor. The other weakness of family medicine is still its relatively lower status, compared to other specialties, in society, profession and academia, which limits its professional and scientific development. There are some unprecedented opportunities for family medicine in Hong Kong. The PHC Blueprint with the advocacy of family doctors for all, the establishment of DHC/E in all 18 districts, the formation of the PHC Commission with dedicated funding for PC and the likely development of the PC Directory into a PC Registry have provided an ideal open system for medical-social-behavioural care integration in primary care led by family doctors. The greatest threat to family medicine is the use of PC as the dumping ground of all sorts of problems, in which family medicine may fail to deliver up to expectation. Many other professionals are crossing their boundaries to PC, which may dilute the ownership and identity of family medicine. The increasing workload and responsibility may put family doctors at risk of burn-out and threaten their mental wellbeing. The Hong Kong College of Family Physicians needs to prepare our family doctors for the new challenges through appropriate training and continuous medical education. Figure 2: SWOT analysis of family medicine in the new era of primary care 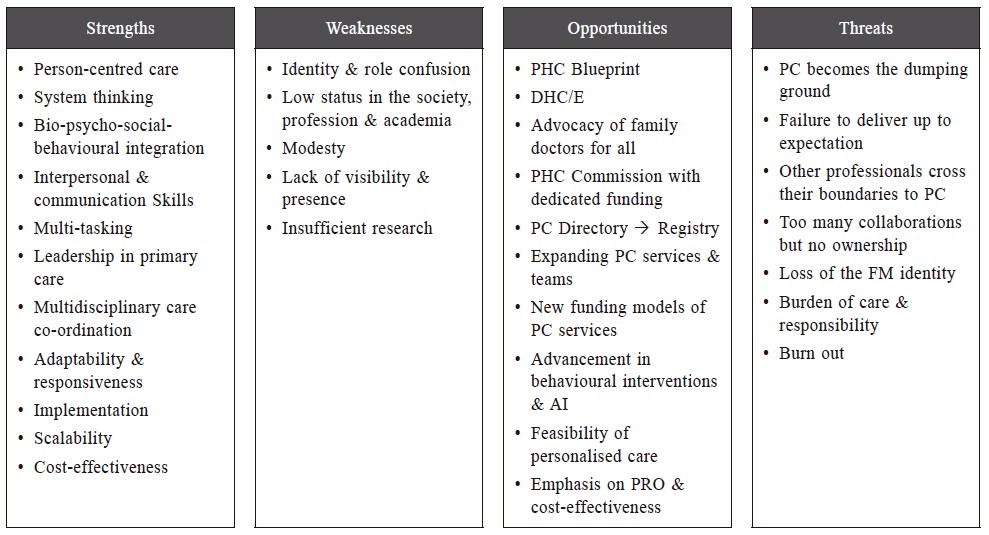
ConclusionPrimary care is becoming more complex with an increasing number of services available to meet the needs of different patients, but more is not necessarily better. Everyone needs a personal family doctor who can connect the right services, including self-care, family support, community resources, healthcare services and social services, to the person at the right time to achieve the best health outcome at the lowest cost.
AcknowledgmentThe KGKF-HKU Health Empowerment Programme for Low-income Families was funded by the HKU Kerry Group & Kuok Foundation (KGKF) Endowed Research Fund. The ethics of the KGKF-HKU Health Empowerment Programme was approved by the IRB of the University of Hong Kong-HA HKWC (Ref. UW 12-517). Special thanks go to all participating families of the KGKF-HKU Health Empowerment Programme. Acknowledgement of the community partners of the KGKF-HKU Health Empowerment Programme in alphabetical order: Mental Health Association of HK (MHAHK), Neighbourhood Advice-Action Council (NAAC), Project Concern HK – Yat Tung Estate Dental Clinic, Sheng Kung Hui Lady MacLehose Centre, Sheng Kung Hui Tung Chung Integrated Services, the HK Federation of Education Workers (HKFEW), the HK Outlying Island Women’s Association (OIWA), the HK Society for Rehabilitation, Tung Chung Catholic School HK (HKSKH), Tung Chung Safe and Healthy City (TCSHC), TWGHs Ko Ho Ning Memorial Primary School, Wong Cho Bau School and Yat Tung (I/II) Estate Property Management. I am grateful for the hard work of the HKU Project Team: Emily Tse, Amy Ng, Kiki Liu, Carlos Wong, Ben Fong, Fangcao Lu, Daniel Fong, Calvin K Or, Patrick Ip, David Lam, Wendy Lam, Virginia Wong, Rainnie Pan, Alice Zheng, Qi Kang and Fleur Lee. References
* This article is adapted from the presentation on “Family Medicine: Connecting the Right Services at the Right Time to the Right Person” at the Hong Kong Primary Care Conference 2024, Hong Kong College of Family Physicians, Hong Kong 5-7 July 2024
Cindy LK Lam,
MBBS (HK), MD (HK), FHKAM (Family Medicine), FRCGP
|
|