
|
December 2024,Volume 46, No.4
|
Update Article
|
Interpreting spine radiographsWilfred CG Peh HK Pract 2024;46:78-95
SummaryAlthough neck and back pain are common symptoms, the vast majority of affected patients will not need imaging of the spine as clinical outcomes are usually not improved, with disadvantages including inappropriate use of resources and unnecessary ionising radiation hazard. This article aims to provide a practical refresher to family physicians - reviewing the indications for spine radiography, approach to interpreting these radiographs, and highlighting the appearances of some common lesions and incidentalomas.Keywords: Ankylosing spondylitis, low back pain, osteoporotic fracture, spine degeneration, spine fracture, spine radiograph, spondylolisthesis, spondylolysis, vertebral compression fracture, vertebral metastasis
摘要雖然頸部和背部疼痛是常見的症狀,但絕大部分病人並不 需要進行脊柱影像學檢查,因為檢查對於改善臨牀症狀並 沒有幫助,而且還會造成資源不當使用以及不必要的輻射 危害。本文旨在於為家庭醫生提供實用的重溫資料,包括 脊柱X光檢查的適應症,如何解讀放射學影像,並且重點 說明一些常見疾病的表現和偶見瘤(影像學檢查中偶然發現 的腫物)。關鍵詞:強直性脊椎炎、下背痛、骨質疏鬆性骨折、脊椎 退化、脊椎骨折、脊椎X光、腰椎滑脫、脊椎裂、脊椎壓 迫性骨折、椎體轉移 IntroductionLow back pain is a common complaint found in patients presenting to family physicians. Imaging of the spine is not required in the vast majority of these patients. Proper utilisation of imaging should result in improved clinical outcomes. Unnecessary imaging leads to increased cost, inappropriate use of resources and most critically, unnecessary ionising radiation hazard. Compared to a chest radiograph which has a typical effective dose of 0.015mSv, a lumbar spine radiograph has a 40-fold higher effective dose of 0.6mSv.1 In contrast to a chest radiograph, the radiation dose to the (nearby) gonads is also considerably higher when obtaining a standard set of two-view anterior-posterior (AP) and lateral radiographs of the lumbosacral spine. While the risk of cancer from relatively small doses of ionising radiation from diagnostic imaging is generally low, there is no dose at which this risk can be completely eliminated. There is a standard radiation protection dictum: the ALARA principle. ALARA is an acronym for keeping radiation doses “As Low As Reasonably Achievable”. The expected benefits of radiation exposure must be balanced against the potential risks, bearing in mind whether the planned imaging examination is able to answer the clinical question. This answer goes beyond just detecting abnormalities and making a diagnosis but more importantly, whether diagnostic imaging undertaken will impact management of the patient. This article aims to provide a practical refresher to family physicians comprising: (1) the indications for imaging the spine, (2) approach to interpreting spine radiographs, and (3) reviewing the appearances of some relevant common lesions. IndicationsThe assessment of a patient presenting with back or neck pain should start with a thorough clinical evaluation looking for “red flags” such as severe or progressive neurological deficits (e.g. cauda equina syndrome, motor loss, bladder dysfunction), infection, cancer, trauma, chronic steroid use, substance abuse and immunosuppression. Non-spinal causes of back pain (e.g. from renal, bowel and pancreatic disease) should also be excluded. Bear in mind that the diagnosis is often elusive even after a careful clinical assessment, and is seldom provided by radiographs alone. Furthermore, presence of asymptomatic incidental findings such as degeneration or spondylolysis may confuse both doctor and patient.2 Currently, magnetic resonance imaging (MRI) is the initial imaging modality recommended for several indications relating to the spine, with computed tomography (CT) also being an appropriate modality, e.g. acute cervical spine trauma, spinal infection. For example, in a patient presenting with pain or neurological deficit after spinal trauma; if radiographs are abnormal, CT and/or MRI is indicated. CT gives detailed analysis of bone injury and MRI is indicated for multilevel, ligamentous and cauda equina injuries. Discussing the roles of MRI, CT and other more advanced imaging modalities e.g. nuclear medicine (NM) studies in investigating spinal lesions is beyond the scope of this article. However, there remains a role for spine radiographs in certain circumstances. Details of the specific indications for performing spine radiographs can be found in excellent referral guidelines/appropriateness criteria published by professional bodies such as the Royal College of Radiologists3 and the American College of Radiology.4-7 Some common indications for performing spine radiographs relevant to family physicians are listed in Table 1. Approach to interpretationBy the time your patient undergoes a set of spine radiographs, your aim will be to confirm your clinical suspicions by the expected detection or exclusion of certain lesions, hopefully positively supporting your management plan. My own system to review spine radiographs is: 1. Check that the region of interest is covered.
Table 1: Common indications for performing spine radiographs3-7Low back pain
Neck pain
Others
Figure 121-year-old man with neck injury. (a) Initial lateral cervical spine radiograph shows normal spinal alignment. However, only the upper 6 vertebra are depicted. (b) Repeat radiograph with shoulders pulled down shows C6/7 subluxation with unilateral facet dislocation. This is a potentially unstable injury as all 3 spinal columns are disrupted. 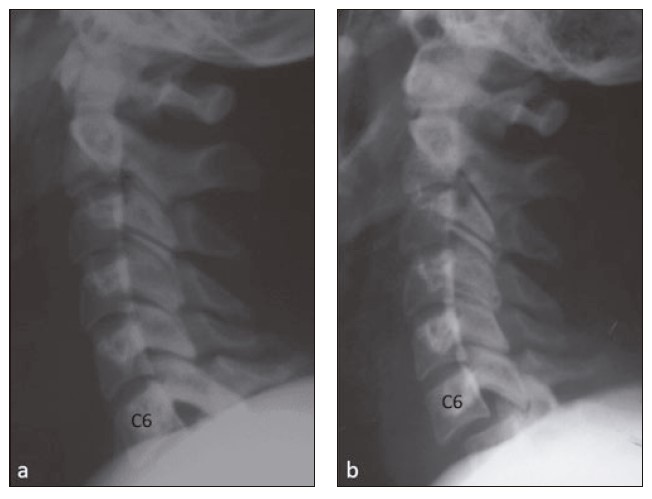
Figure 2Lateral long-spine radiograph shows normal cervical lordotic, thoracic kyphotic and lumbar lordotic curves. Curves change direction at the cervicothoracic ( thin arrow ) and thoracolumbar ( thick arrow ) junctions. 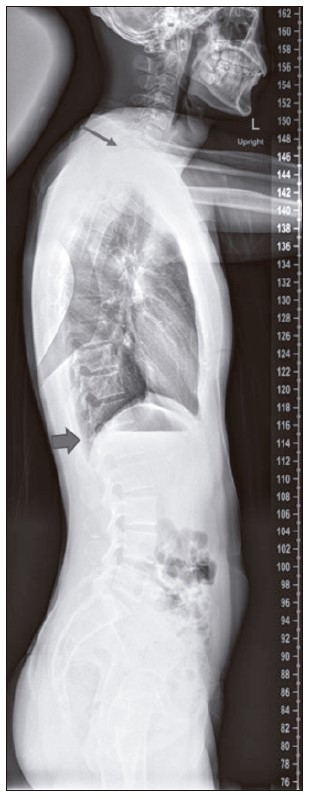
2. Are additional radiographic projections required?
3. Look at the anatomical components of the spine systemically.
Figure 3Normal cervical spine radiographs. (a) Lateral projection shows a normal lordotic curve and the 5 spinal lines are marked. Line 1: Pre-vertebral soft tissue thickness should not exceed 5mm at C1-4 levels (asterisks) and not exceed one vertebral body AP width at C5-7 levels (double arrows). Line 2: Anterior spinal line (2) that links the anterior cortices of the vertebral bodies should form a smooth continuous curve. Line 3: Posterior spinal line (3) that links the posterior cortices of the vertebral bodies should form a smooth continuous curve. Line 4: Spinolaminar line (4) that links the junctions between the laminae (L) and bases of the spinous processes should form a smooth continuous curve. Spinal lines 2-4 should be parallel. Line 5: Check that the spinous processes (S) are intact. (b) AP projection shows the C5/6 uncovertebral joints (small arrows), C6 pedicles (arrowheads) and the C6 and T1 spinal processes (S). 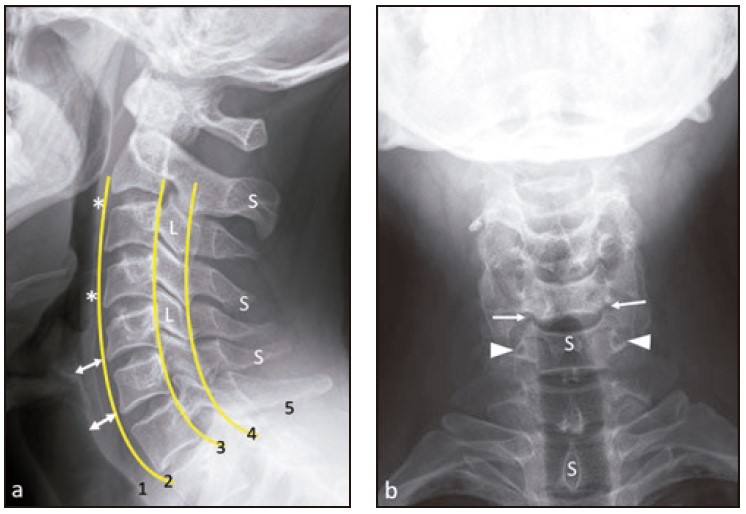
Figure 4Transitional lumbosacral segment with L5 sacralisation. (a) AP and (b) lateral lumbosacral spine radiographs show that the L5 vertebra (L5) is sacralised. Well-formed 12th ribs (R) indicate the T12 vertebral body (T12). Some anatomical structures are labelled: L3/4 intervertebral disc (*), L4 pedicles (P), L4 spinous process (S), right L2/3 facet joint (small arrows), left L2 inferior articular process (I), left L3 superior articular process (arrowhead) and the L2/3 intervertebral neural foramen (F). Both sacroiliac joints are normal (thick arrows). 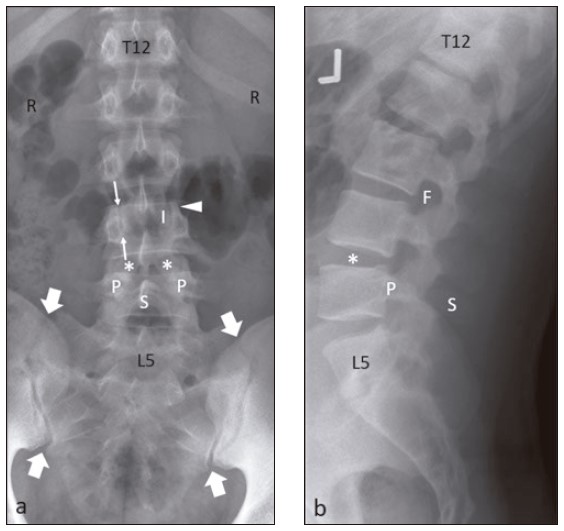
Figure 5Transitional lumbosacral segment with S1 lumbarisation. (a) AP and (b) lateral lumbosacral spine radiographs show that the sacral S1 segment is lumbarised (S1). Well-formed 12 ribs (R) indicate the T12 vertebral body (T12). The L5 vertebral body is labelled (L5). 
Common lesionsIn this section, I have listed some common spinal lesions that may be encountered in the setting of a community-based practice, and therefore relevant to family physicians. When patients with suspected spinal diseases are referred for imaging, clinicians should be seeking answers as to what the cause of the patient’s pain or neurological symptoms is, and considering what the potential treatment options are. The imaging findings should therefore always be interpreted in the context of the patient’s clinical condition. A vertebral fracture is diagnosed when there is at least 20% vertebral body height loss radiographically. The vertebra is the most common location for osteoporotic fracture, and usually results from minor trauma, typically in an elderly woman. This may affect the anterior, middle or posterior portions of the vertebral body. Anterior vertebral body fractures are the most common type and are known as wedge fractures (Figure 7). Fractures involving the middle portion of the vertebral body are also called end-plate or codfish fractures, due to its shape. Vertebra plana (crush fracture) occurs when all three portions show severe height loss and are the least common type.8 Figure 6Oblique radiograph of the lumbar spine. Some anatomical structures relating to L3 vertebra, producing the shape of the front of a Scottie dog, are labelled. The thick blue arrow points to the L3 transverse process (nose of the Scottie dog). L3 pedicle (white eye of the Scottie dog) ; L3 superior articular process (ear of the Scottie dog) ; L3 inferior articular process ( front leg of the Scottie dog ) ; L3 parsinterarticularis (red collar of the Scottie dog). L2/3 facet joint (short arrow), L3/4 facet joint (long arrow) and L3/4 intervertebral disc (*). 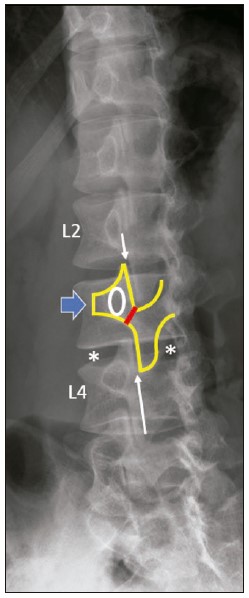
Distinguishing between acute osteoporotic and pathological vertebral compression fractures may be difficult. Radiographical features which tend to favour a benign vertebral fracture are: no bone destruction, no convex bulging of the posterior cortex, retropulsed fragment(s) and multiple compression fractures. History of or finding a known primary malignancy or knowledge of metastases elsewhere are very helpful in supporting the diagnosis of a pathological fracture. Radiographical features of osteoporosis consist of increased vertebral radiolucency and cortical thinning with a “picture framing” appearance. The latter feature is best seen on lateral radiographs and is due to the cortex appearing relatively sharp compared with the trabeculae appearing more radiolucent due to osteoporotic bone resorption8 (Figure 8). MRI is usually indicated to discriminate between acute osteoporotic and pathological fractures and if needed, image-guided biopsy may be required (Figure 9). Figure 7Osteoporotic T12 compression fracture in a 79-year-old woman who fell onto her back. (a) Initial lateral lumbosacral spine radiograph shows mild T12 vertebral body compression fracture, with superior end-plate depression. (b) Follow-up lateral radiograph taken 3 weeks later shows progression to severe wedge compression affecting mainly the anterior and middle portions of the T10 vertebral body. Superior end-plate sclerosis is due to callus. All the bones are osteoporotic. Incidental finding of a calcified abdominal aorta (A) 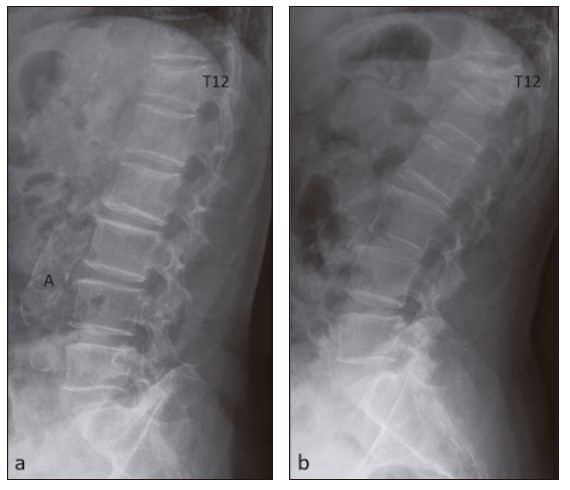
Figure 8Osteoporotic L1 compression fracture in a 63-year-old woman who presented with low back pain. (a) Initial lateral lumbosacral spine radiograph shows mild L1 vertebral body compression fracture with an anterior cortical break (arrow). (b) Follow-up lateral radiograph taken 6 weeks later shows progression to moderate compression with superior end-plate sclerosis. Vertebral bodies are generally osteoporotic, with sharp thin cortical outlines and relative trabecular lucency, giving a “picture framing” appearance. 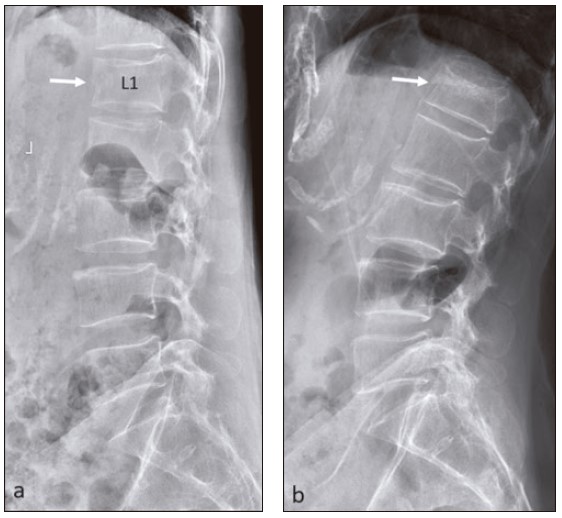
Traumatic spinal fractures usually result from significant trauma (e.g. road traffic accident, fall from height) and are not often encountered in the family practice setting. A wide variety of traumatic fractures can occur, depending on factors such as spinal location, anatomical site and mechanism of injury (Figures 10 & 11) . In assessment of spinal fractures, it is important to try to determine whether the injury is stable or unstable. The three-column concept of thoracolumbar spinal fractures originally advocated by Denis forms the basis for many spinal fracture classification systems. In short, a spinal segment is considered unstable when injuries affect two contiguous columns (anterior and middle column, or middle and posterior column), or if all three columns are injured (Figures 1, 10 & 11). Vertebral metastases usually result from haematogenous spread from a known primary tumour, with common ones being breast, lung, prostate and kidney. They are much more often found in older patients (>50 years old). Within the spine, most metastases are located in the lumbar vertebrae. Radiographically, metastases may appear osteolytic, osteoblastic or mixed (particularly if treated). Primary tumours typically producing osteolytic or predominantly osteolytic metastases are breast, lung, thyroid and kidney; while the classical primary tumours producing osteoblastic metastases are prostate carcinoma and osteogenic sarcoma. On radiographs, metastasis can range in appearance from being invisible to gross destruction, typically involving the posterior vertebral body and pedicles9 (Figures 12 & 13). Degenerative changes in the spine are very common. These changes increase with age and are virtually ubiquitous in late adulthood, so much so that they are regarded as part and parcel of the ageing process. As the presence of degenerative changes is not itself an indicator of symptoms, the imaging findings of spinal degeneration must be interpreted bearing in mind the patient’s clinical context. Degenerative disease of the spine most commonly involves the lumbar spine, followed by the cervical spine. On radiographs, vertebral body end-plate hypertrophy manifesting as osteophyte formation and loss of intervertebral disc height (inferring disc degeneration) are seen, followed later on with more advanced degenerative changes such as end-plate sclerosis and irregularity, facet joint osteoarthritis and spinal canal stenosis (Figures 10, 14, 15, 16 & 17) . In the cervical spine, look out for degenerative changes involving uncovertebral joints on the AP radiograph10 (Figures 10 & 16). Figure 9Osteoporotic L1 and L2 compression fractures in a 73-year-old woman who presented with low back pain and suspicion of fracture. Initial (a) AP and (b) lateral lumbosacral spine radiographs show L1 and L2 vertebral body compression fractures (thin arrows). Sagittal (c) T1-and (d) T2-weighted MR images show the L2 fracture to be acute and L1 fracture to be chronic. Normal marrow signal is present in the L1 vertebral body, while there is abnormal oedematous signal around a fracture line in the L2 vertebral body. There are no features of malignancy. (e) Follow-up lateral lumbosacral spine radiograph taken 3 months later shows further L2 vertebral body compression with dense sclerosis indicating healing. No change in appearance of the chronic L1 vertebral fracture. Incidental finding of a dense calcified uterine fibroid in the pelvis (thick arrows). 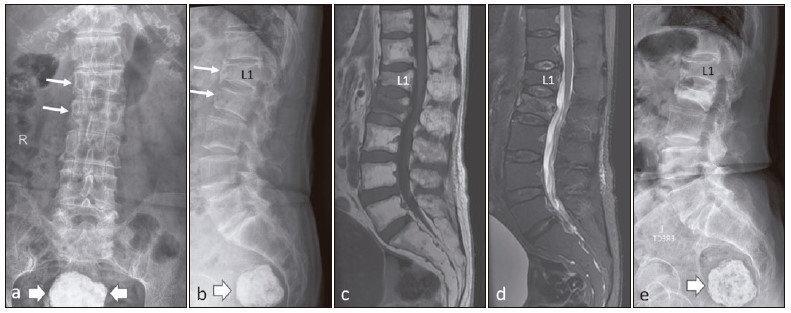
Figure 10Acute traumatic odontoid fracture in a 70-year-old man who presented with neck pain after a fall. (a) Lateral cervical spine radiograph shows a mild displaced odontoid peg fracture (arrows). There is loss of normal cervical lordosis with mild lower cervical kyphotic deformity. Moderate C4-7 degeneration is present, with small anterior and posterior osteophytes, and narrowing of the C4-7 intervertebral disc spaces. (b) AP cervical spine radiograph shows C4-7 uncovertebral joint degenerative changes but the odontoid peg is obscured by the mandible. (c) Open mouth AP radiograph shows the mildly displaced odontoid fracture (arrows). 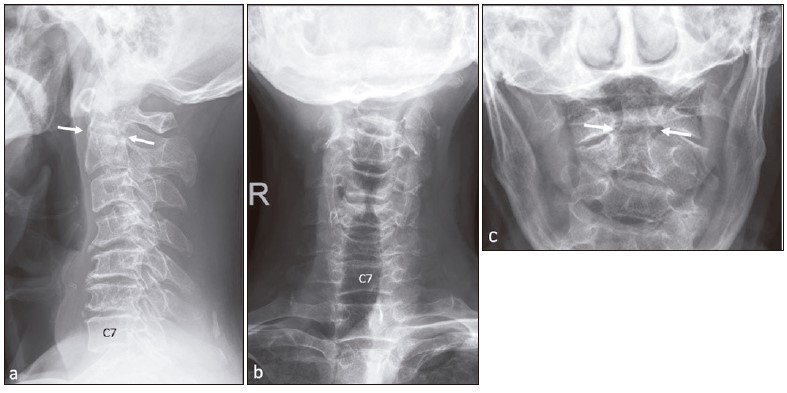
Figure 11Acute traumatic L4 burst and L5 pars fractures in a 38-year-old man who presented after trauma to back. Initial (a) lateral and (b) AP lumbosacral spine radiographs show a L4 burst fracture with L4/5 retrolisthesis and L5/S1 anterolithesis. There is a large L4 posterior retropulsed fragment (thick arrow) and splaying of both L4 pedicles (arrows). Bilateral L5 pars fractures are present (arrowheads). This spinal injury is clearly unstable as all 3 (anterior, middle and posterior) vertebral columns are disrupted. Follow-up (c) lateral and (d) AP radiographs after L2-S1 posterior spinal fusion show restoration of spinal alignment. There are numerous embolisation coils. 
Figure 12Multiple osteoblastic metastases in an 82-year-old man, known to have prostatic carcinoma, who presented with low back pain. (a) Lateral and (b) AP lumbosacral spine radiographs show multiple osteoblastic metastases affecting the L2-5 vertebral bodies, with involvement of both L3 and left L4 pedicles, sacrum, right and left ilia, left acetabulum, right superior pubic ramus. Incidental finding of mild L1 wedge compression fracture, likely osteoporotic. 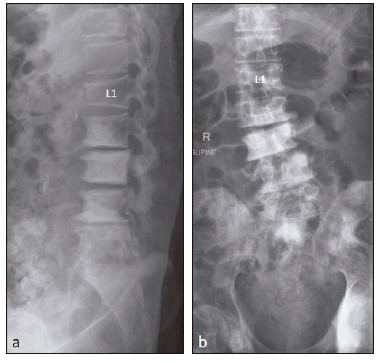
Degenerative spondylolisthesis is most commonly seen in the lumbar spine, followed by the cervical spine and is uncommon in the thoracic spine . Spondylolisthesis formation is thought to result from severe disc degeneration (Figure 18). Degenerative spondylolisthesis can be divided into dynamic spondylolisthesis and the static subtype, with the former showing instability on flexion/extension radiographs (Figures 19 & 20) . Thi s additional diagnostic information may alter patient management, particularly when surgery is being considered.10 Figure 13Osteolytic metastasis in a 65-year-old woman who presented with back pain. (a) AP and (b) lateral thoracic spine radiographs show a T10 compression fracture with osteolytic destruction and paraspinal soft tissue swelling (arrowheads). Note splaying of the remnant T10 vertebra body (arrows), with mild levoscoliosis centered at the collapsed vertebra. She was subsequently found to have breast carcinoma. Follow-up (c) AP and (d) lateral radiographs after T10 decompression and T7-L1 posterior spinal fusion show positions of the posterior instrumentation screws and rods. Incidental finding of calcified gallstones (small thick arrows) 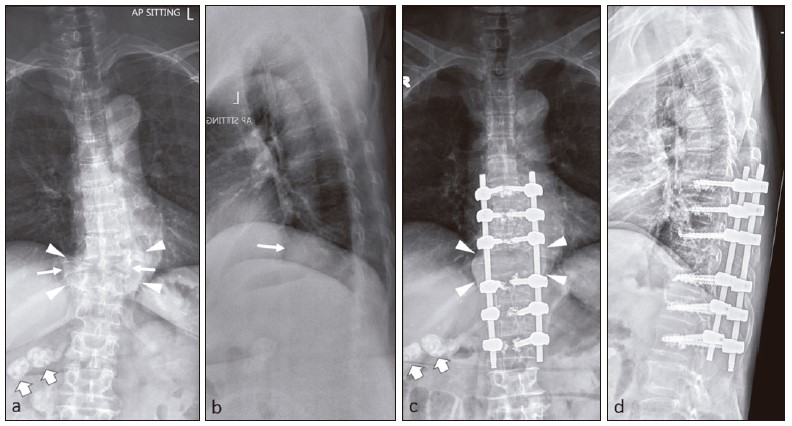
Spondylolysis refers to a defect in the pars interarticularis, which is the portion of the neural arch connecting the superior and inferior articular facets (Figure 6). It also known more simply as a pars defect. Spondylolysis occurs most commonly at the 5th lumbar vertebra. The lateral radiograph is sensitive for detection of pars defect, with the oblique views being more specific. On oblique lumbar radiographs, the posterior elements form the appearance of a Scottie dog, with the pars interarticularis defect giving the appearance of a collar around the neck (Figure 6). Spondylolysis may be developmental or acquired. Developmental defects occur in patients less than 10 years of age. Acquired pars defects have two main mechanisms: (a) repeated microtrauma, resulting in a stress injury and eventual fracture, with a dysplastic pars usually present; and (b) traumatic pars defects resulting from high-energy trauma where there is hyperextension of the lumbar spine11 (Figures 11, 21 & 22). Many patients with spinal disorders that cannot be managed conservatively undergo spinal surgery. In patients who have had spinal instrumentation surgery, radiographs can be used to determine the position of the implants, progression of osseous fusion, and to diagnose complications such as fractures and adjacent segment degeneration. Comparison of follow-up radiographic findings to baseline postoperative radiographic findings helps detect changes in device position and loss of implant fixation12 (Figures 11, 13, 18 & 23). Ankylosing spondylitis is a rare, chronic and progressive form of seronegative arthritis that has a predilection for the axial skeleton. I t affects particularly the sacroiliac and spinal facet joints, and paravertebral soft tissues. Radiographs are the single most important imaging technique for the detection, diagnosis, and follow-up monitoring of patients with ankylosing spondylitis. Radiographs of the sacroiliac joints is usually the first imaging modality to diagnose sacroiliitis as part of axial spondyloarthropathy. Sacroiliitis is typically symmetrical and bilateral, with radiographical findings of sacroiliac joint narrowing, subchondral erosions and sclerosis on the iliac side of the sacroiliac joints. In end-stage disease, the sacroiliac joint fuses and may be seen as a thin line or is not visible. In the vertebra, early spondylitis is characterised by small erosions at the corners of vertebral bodies with reactive sclerosis (shiny corner sign). Other features include vertebral body squaring, syndesmophytes (seen as paravertebral ossification running parallel to the spine), diffuse syndesmophytic ankylosis giving a "bamboo spine" appearance, and ossification of spinal ligaments, joints and discs, apophyseal and costovertebral arthritis and ankyloses, and enthesophyte formation13 (Figures 24 & 25). Figure 14Mild lumbar spine degeneration in a 72-year-old man who presented with low back pain. (a) Lateral and (b) AP lumbosacral spine radiographs show small anterior and lateral osteophytes at L1-S1 levels. All the intervertebral disc spaces are preserved. Incidental finding of a calcified abdominal aorta (A). 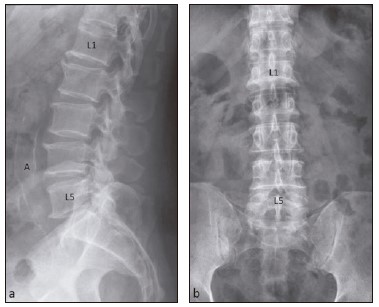
Figure 15Moderate thoracic spine degeneration in a 75-year-old man who presented with neck and back pain. (a) Lateral and (b) AP thoracic spine radiographs show small anterior and lateral osteophytes throughout the thoracic spine with several levels of mild intervertebral disc space narrowing in the lower thoracic spine (arrowheads). There is mild thoracolumbar levoscoliosis. This patient also had moderate degeneration of the cervical and lumbar spine (not shown). 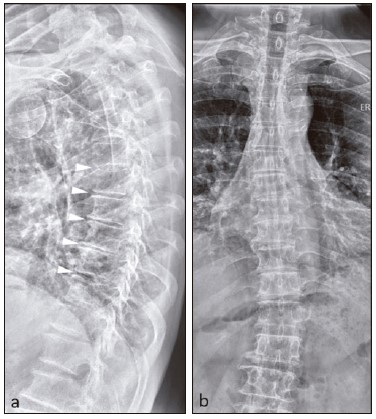
Figure 16Moderate cervical spine degeneration in an 80-year-old man who presented after a fall. (a) Lateral cervical spine radiograph shows loss of normal cervical lordosis with cervical kyphotic deformity. Only the upper 5 cervical vertebrae are visible, showing prominent anterior and small posterior osteophytes at C3-5 levels, with mild C3/4 and C4/5 disc space narrowing. (b) AP cervical spine radiograph shows bilateral uncovertebral joint degenerative changes at C3-6 levels, manifesting as osteophytic lipping, joint narrowing and subchondral sclerosis (arrows). 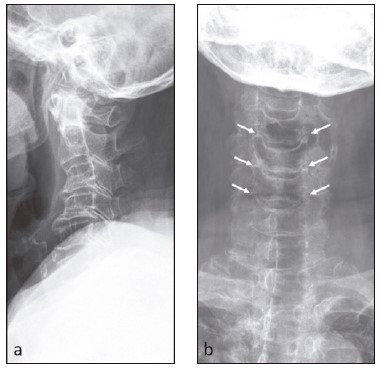
Figure 17Severe lumbosacral spine degeneration in a 68-year-old man who presented with low back pain. (a) Lateral and (b) AP lumbosacral spine radiographs show features of severe L5/S1 degeneration, comprising moderately large anterior osteophytes, small posterior osteophytes, severe disc space narrowing, end-plate subchondral sclerosis (arrows), and hypertrophic facet degeneration (arrowhead). Incidental finding of a calcified abdominal aorta (A). 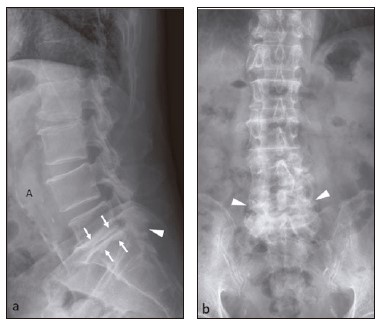
Figure 18Degenerative spondylolisthesis in a 61-year-old man who presented with neck pain. Initial (a) lateral and (b) AP cervical spine radiographs show mild loss of cervical lordosis, moderate C5/6 and C6/7 anterior and posterior osteophytes, mild C6/7 anterolisthesis (arrowhead) with C5/6 and C6/7 intervertebral disc space narrowing, worse at C6/7 level. There is C7/T1 facet degeneration. Follow-up (c) lateral and (d) AP radiographs following anterior cervical discectomy and fusion show C5-7 plate and screws with C5/6 and C6/7 disc implants. Alignment is restored. 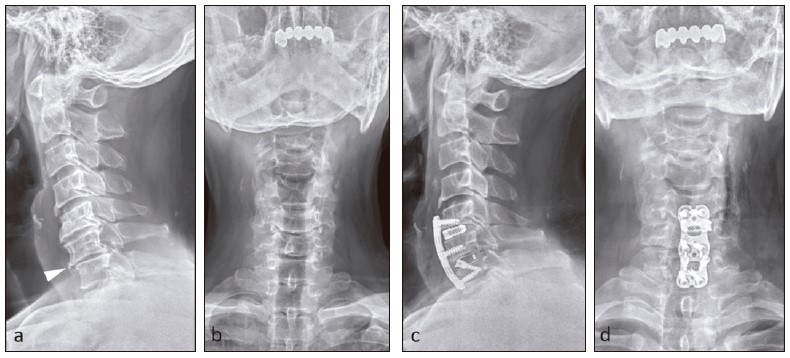
Figure 19Mild L4/5 spondylolisthesis in a 67-year old man who presented with low back pain. Upright lateral lumbosacral spine radiographs taken in (a) neutral, (b) extension and (c) flexion positions show L4/5 anterolisthesis that is worse on flexion (arrowheads). The L4/5 disc space is narrowed and there is L4/5 facet degeneration (arrow). 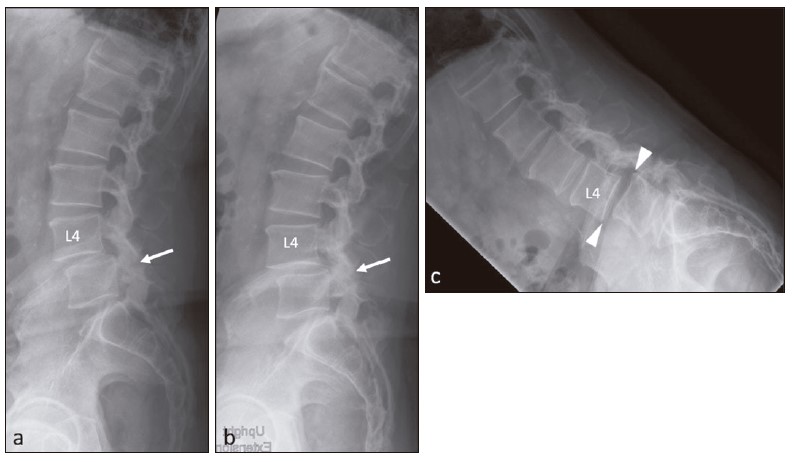
Figure 20Development of L3/4 spondylolisthesis in a 53-year-old man who presented with low back pain and worsening radiculopathy post-operatively. Patient underwent L3/4 decompression. Pre-operative (a) AP and (b) lateral lumbosacral spine radiographs show maintenance of spinal alignment. Follow-up lateral radiographs obtained 8 weeks post-operatively taken in (c) extension and (d) flexion positions show L3/4 anterolisthesis only on flexion (arrowheads). 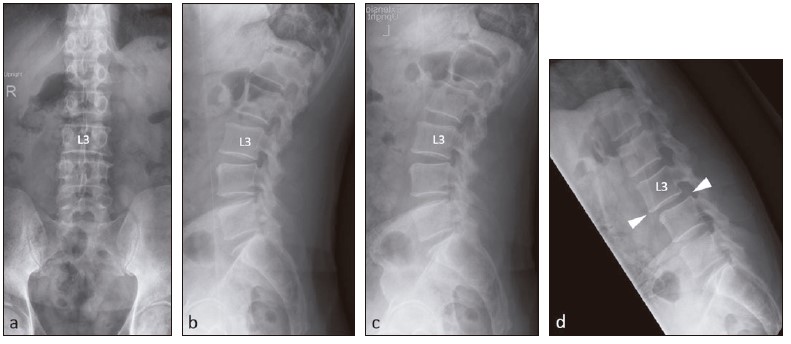
Figure 21Slight L5/S1 spondylolisthesis due to bilateral L5 pars defects in a 26-year-old woman who presented with low back pain. (a) AP and (b) lateral lumbosacral spine radiographs show slight L5/S1 anterolisthesis (arrowhead) due to bilateral L5 pars defects (arrow). (c) Lateral radiograph taken in extension better shows the L5 pars defects (arrow) as well as more pronounced L5/S1 anterolisthesis (arrowhead). 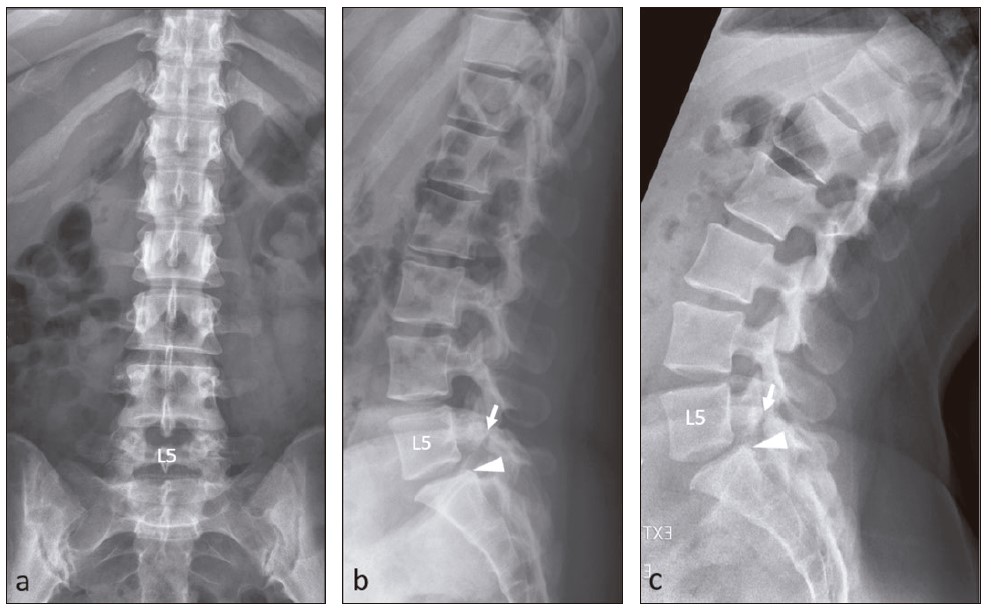
Figure 22Progression of L5/S1 spondylolisthesis due to bilateral L5 pars defects in a 47-year-old man who presented with back pain and left S1 radiculopathy. (a) Initial lateral lumbosacral spine radiograph shows mild L5/S1 anterolisthesis due to bilateral pars defects (arrow). The L5/S1 intervertebral disc space is moderately narrowed. Repeat erect (b) neutral and (c) flexion lateral radiographs taken 2 years later show progression of L5/S1 anterolisthesis. There is more marked L5/S1 disc space narrowing with further osteophyte formation (thick arrow). The L5 pars defect appears widened on flexion (arrow). 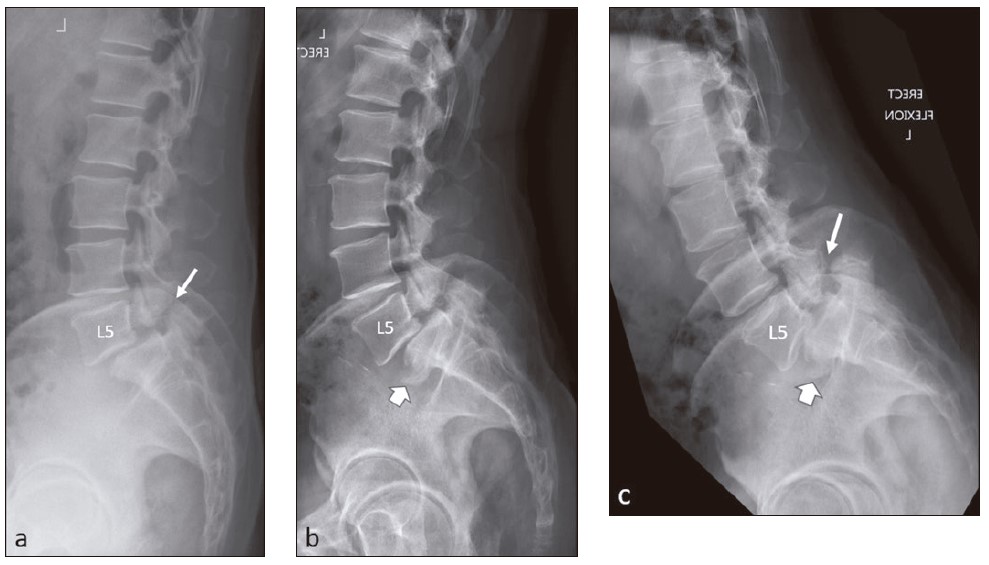
Figure 23Mild spondylolisthesis after L4/5 posterior spinal fusion in a 59-year-old woman. (a) Lateral and (b) AP lumbosacral spine radiographs show L4/5 posterior instrumentation screws and rods with intervertebral disc replacement. There is mild L4/5 anterolisthesis. Incidental findings of numerous small dense phosphate binders scattered within the bowel and a calcified abdominal aorta (A). 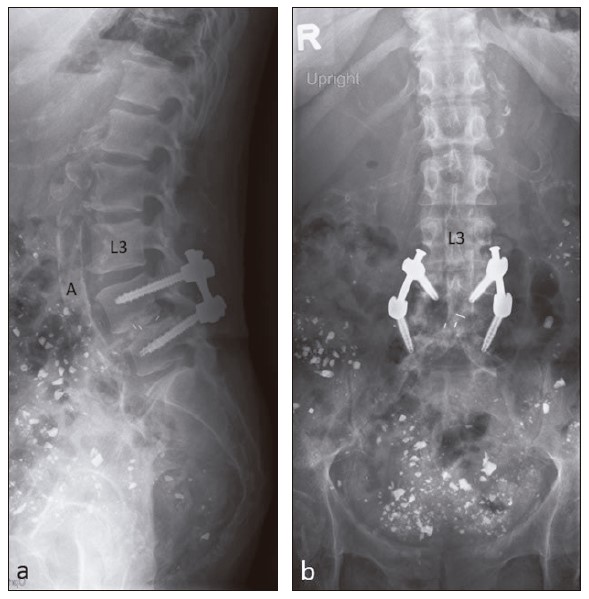
Figure 24Early ankylosing spondylitis in a 23-year-old man who presented with back pain. (a) Lateral and (b) AP lumbosacral spine radiographs show bilateral sacroiliitis. Both sacroiliac joints are irregular, with marginal erosions, worse on the right. There is bilateral iliac-sided subchondral sclerosis, worse on the right (arrows). (c) Right oblique radiograph confirms the typical appearances of sacroiliitis, with prominent subchondral sclerosis (arrows). Note that the vertebral bodies and facet joints are normal, consistent with early ankylosing spondylitis. There is no ligamentous ossification yet. 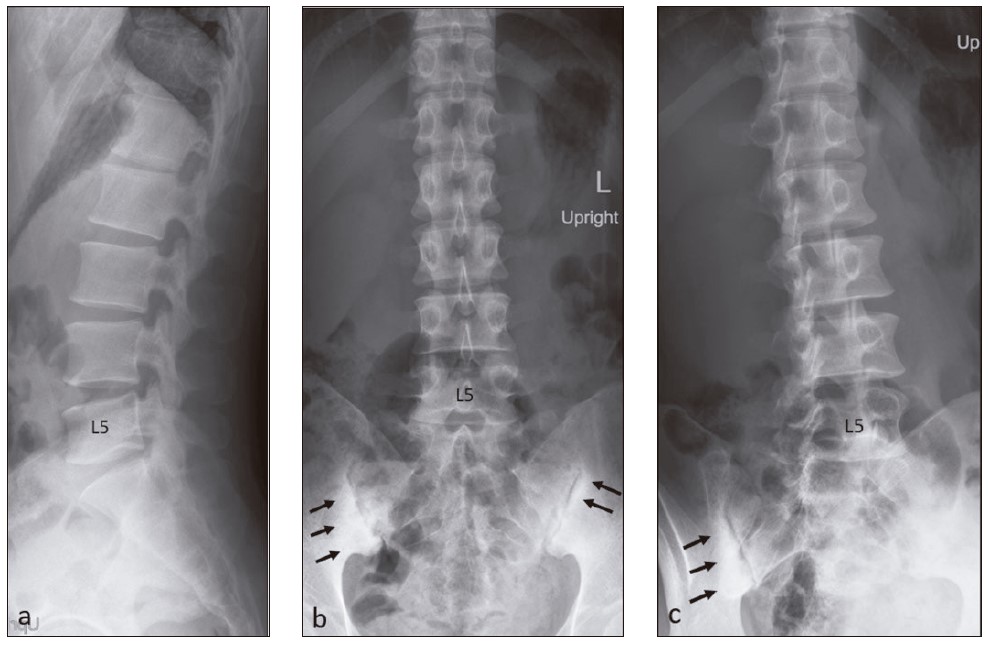
Figure 25Well-established ankylosing spondylitis in a 37-year-old man. ( a ) AP and ( b ) lateral lumbosacral spine radiographs show complete ankylosis of both sacroiliac joints. Extensive syndesmophyte formation (arrowheads) produce a “bamboo spine” appearance and there is fusion of all the lumbar facet joints (thick arrows). Both iliolumbar ligaments are ossified (thin arrows). 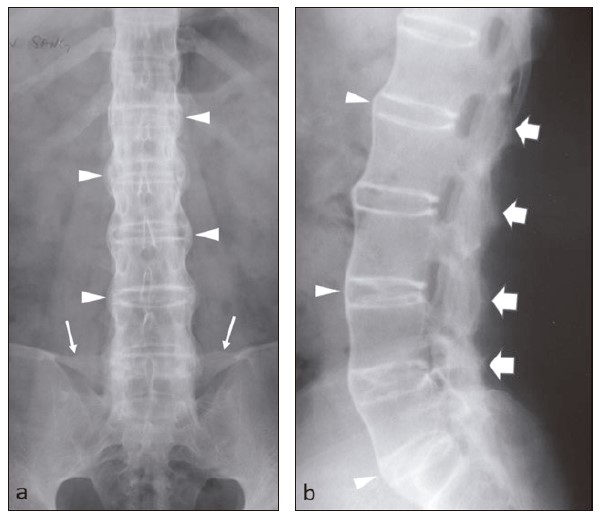
Figure 26Diffuse idiopathic skeletal hyperostosis (DISH) found incidentally in a 66-year-old man who presented with suspected foreign body in his throat. (a) Lateral neck radiograph shows incidental finding of flowing ossification affecting the anterior vertebral bodies at C2-7 levels. The interverterbral disc spaces are generally normal in height. (b) Sagittal CT image shows all these findings better and shows the full extent of DISH (C2-T3 levels). 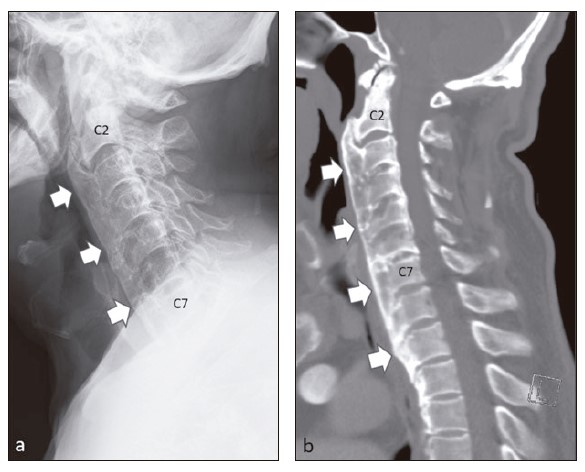
Figure 27Thoracolumbar scoliosis in a 20-year-old man who presented with back pain. AP long-spine radiograph shows a moderate primary curve in the mid-thoracic region, convex to the right (dextroscoliosis)., with the secondary curve at the upper lumbar region, convex to the left (levoscoliosis). There is no vertebral anomaly. 
Figure 28Spina bifida occulta found incidentally in a 37-year-old woman who presented with cervical radiculopathy. AP cervical spine radiograph shows a well-corticated defect in the T1 neural arch, close to the midline (arrows). Subsequent MRI did not reveal any other abnormality. 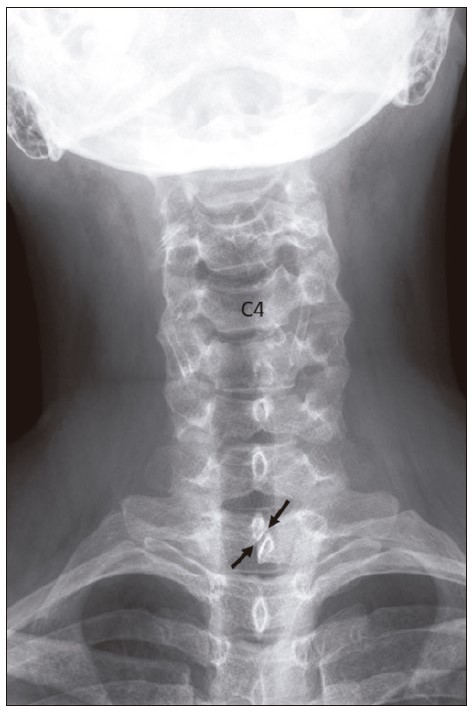
Figure 29Accessory spinous process ossicles found incidentally in a 33-year-old man who presented with neck pain after a road traffic accident. Lateral cervical spine radiograph shows well-corticated fragments (arrows) separated from the tips of the C7 and T1 spinous processes by a narrow vertical gap . The adjacent spinous processes are also well corticated, indicating the longs tanding nature of these ossicles. The C7 accessory ossicle is better visualised than the T1 ossicle due to the soft tissue bulk of the shoulders partially obscuring the latter. 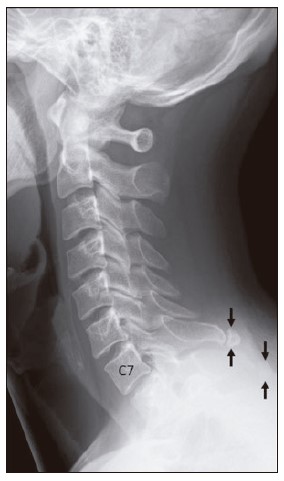
Figure 30Limbus vertebra in a 20-year-old woman who presented with persistent back pain. Lateral lumbosacral spine radiograph shows a well-defined and corticated fragment at the antero-superior corner of L3 vertebral body. The fragment is triangular in shape and arises from a defect in the adjacent vertebral body. The defect is well-corticated with sclerotic margins, indicating chronicity. 
Diffuse idiopathic skeletal hyperostosis (DISH) of the spine (or Forestier disease) is characterised by continuous coarse thickened bony bridging along the anterior longitudinal ligament. The flowing ossification should encompass at least four vertebral bodies, with preservation of the intervertebral disc space. Patients are often asymptomatic and DISH is often discovered incidentally, although symptoms such as neck pain and stiffness may occur (Figure 26). Scoliosis is defined as an abnormal lateral curvature of the spine. It is quite common in young individuals, and is often idiopathic and asymptomatic. In some cases, it results from underlying structural or neurological abnormalities. The most pronounced curve is usually the one at which the main structural abnormality is present, and is termed the primary or structural curve. Scoliotic curves may be described as levoscoliosis (curvature towards the left) or dextroscoliosis (curvature towards the right). Assessment and monitoring of scoliosis is usually achieved with long-spine radiographs, looking for structural osseous abnormalities such as vertebral body wedging, segmentation abnormalities (e.g. hemivertebrae), spina bifida or destructive lesions (Figures 13, 15 & 27). Spina bifida refers to defective fusion of the vertebral posterior neural arch, leading to a bifid osseous configuration. Associated syndromes and anomalies can occur in a minority of cases, including central nervous system and limb anomalies. The lumbosacral region is the commonest site of spina bifida. Spinda bifida occulta is the commonest form of spina bifida; it is usually asymptomatic as there is overlying skin covering the vertebral defect and no associated developmental abnormality of the cord or nerve roots. On the AP radiograph, it appears as a midline or para-midline bony defect of the posterior neural arch (Figure 28). There are five secondary ossification centres in each vertebra from 3rd cervical to 5th lumbar levels. They appear at puberty and fuse by 25-30 years. These are located at: (1) the tip of the spinous process,(2) the tips of each transverse process (two in total) and (3) ring (or annular) apophyses at the upper and lower surfaces of the vertebral bodies (two in total). Accessory ossicle of the spinous process results from non-fusion of the secondary ossification centre located at the tip of the spinous process. On the lateral radiograph, it appears as a well-corticated fragment separated from the spinous process by a vertical or near-vertical lucent margin. Recognising this entity is important in patients presenting with potentially traumatic spinal injuries, where this normal variant should be identified, hence avoiding the potential pitfall of diagnosing a fracture. Its well-defined cortical margin is a helpful clue (Figure 29). Figure 31L4 compression fracture with incidental finding of gallstones in a 58-year-old man who presented with low back pain after a fall. (a) AP and (b) lateral lumbosacral spine radiographs show mild compression of L4 vertebral body (thin arrow). There are cortical breaks in the anterior and posterior margins, as well as the superior end-plate of the vertebral body. No retropulsion is seen. Several calcified gallstones seen in the right upper quadrant on the AP radiograph are projected anteriorly on the lateral radiograph, correlating to the right hypochondriac location of the gallstones (thick arrows). 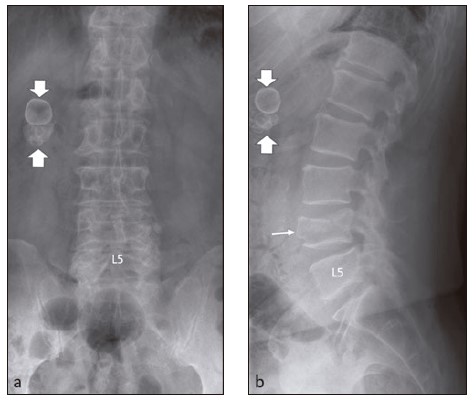
Figure 32T12 compression fracture and incidental finding of renal calculi in an 80-year-old man who presented with low back pain after a fall. (a) AP and (b) lateral lumbosacral spine radiographs show mild anterior wedge compression of T12 vertebral body (thin arrow). There are also mild degenerative changes throughout the lumbar spine and lower thoracic spine. Small rounded dense opacities seen at the right paraspinal region on the AP radiograph corresponds to the retroperitoneal position of the right kidney on the lateral radiograph (arrowheads). 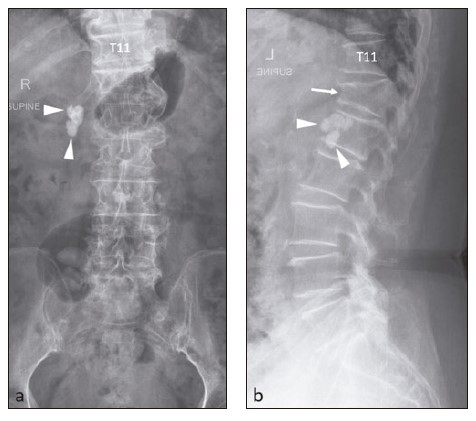
Figure 33Osteoporotic thoracolumbar compression fractures and incidental finding of previous pulmonary tuberculosis in an 85-year-old man who was known to be osteoporotic. (a) AP and (b) lateral thoracic spine radiographs show mild compression of T12 and L1 vertebral bodies (arrows). Mild degenerative changes are present throughout the thoracic spine. There is scarring of the upper zone of the right lung with apical pleural thickening (arrowheads). 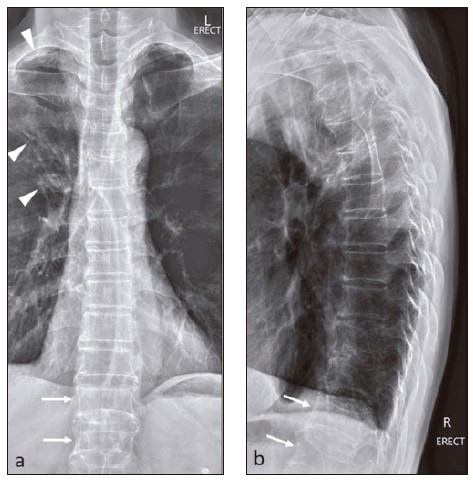
Limbus vertebra refers to a well-corticated unfused secondary ossification centre of the vertebral body, usually found at its anterosuperior corner. It is caused by an old injury in the immature skeleton, resulting in herniation of the nucleus pulposus through the ring apophysis before fusion, with resultant separation from the rest of the vertebral body. A limbus vertebra usually occurs before 18 years of age, but are often seen in older adults. Anterior limbus vertebrae are generally asymptomatic and are detected incidentally. On lateral radiograph, a limbus vertebra is typically wellcorticated, triangular in shape and occupies the expected location of a normal vertebral body corner, adjacent to a smooth, corticated vertebral body margin (Figure 30). 
Besides congenital incidentalomas in the spine such as spina bifida occulta and spinous process accessory ossicle, several other incidental findings may be discovered during the course of obtaining spine radiographs. Some of these non-spinal abnormalities may be insignificant while others may potentially be the cause of the patient’s back or neck pain, such as calcified abdominal aorta (Figures 7, 14, 17 & 23), uterine fibroids (Figure 9), gallstones (Figures 13 & 31), renal calculi (Figure 32), ingested phosphate binders (Figure 23) and even pulmonary tuberculosis (Figure 33). SummaryIn order to optimise the clinical utilisation of spine radiographs in patients presenting with neck or back pain, family physicians should be familiar with the clinical indications. A systematic approach to interpreting spine radiographs is recommended and it is helpful to know the appearances of some common spine lesions and incidentalomas. References
Wilfred CG Peh,
MD (Hong Kong), FRCPG, FRCPEd, FRCR
Correspondence to: Professor Wilfred CG Peh, Senior Consultant, Department of
|
|