
|
September 2024,Volume 46, No.3
|
Case Report
|
Insulin therapy for type 2 diabetes mellitus in primary care – common case scenarios and practical tipsDerek GC Ying 邢格政,Catherine XR Chen 陳曉瑞 HK Pract 2024;46:62-67 SummaryUse of insulin in addition to oral hypoglycaemic agents (OHAs) in the treatment of type 2 diabetes mellitus (T2DM) can be effective, simple and safe in primary care settings by adopting a systematic approach. In this article, we shared three T2DM cases commonly encountered in primary care requiring insulin treatment. First, when and how basal insulin therapy is initiated and titrated are discussed. Hypoglycaemia is uncommon on initiation of insulin, but may gradually appear as insulin is up titrated. We go through how to manoeuvre insulin regimen in case of hypoglycaemia and on sick days. Lastly, we will also explore when to stop further up titration in primary care settings and to consider referral to endocrinologists for further management.
摘要在口服降糖藥物之上規範地使用胰島素,是基層醫療 治療2 型糖尿病的簡單、有效而安全的方法。本文章分享 了三例在基層醫療中常見,與胰島素治療相關的2 型糖尿 病病例。我們會討論何時以及如何使用基礎胰島素。低血 糖反應在剛開始使用胰島素時並不常見,但會隨著治療時 間增加而逐漸浮現。我們會介紹在低血糖反應以及患其他 急病的情況下,如何調整胰島素治療方案。最後,我們會 探討何時應該停止增加胰島素劑量,並考慮轉診于內分泌 科醫生進行。 IntroductionType 2 diabetes mellitus (T2DM) is a chronic disease characterised by insulin resistance and progressive ß-cell dysfunction. The progressive nature of T2DM denotes that the need for insulin would ultimately arise for many patients in order to achieve their glycaemic targets. In Hong Kong, with our ageing population, the number of T2DM patients indicated for insulin treatment has increased over the years. A significant proportion of them are regularly followed up via the General Out-patient Clinics (GOPCs) of the Hospital Authority and are cared for by primary care physicians (PCPs). With the availability of newer insulin analogues and structured risk assessment and management programmes, insulin initiation and intensification can be simple and safe in primary care settings. In this article, we present 3 clinical cases with 7 different scenarios commonly encountered by PCPs when managing T2DM. First, we will discuss the issue of when and how insulin therapy is commenced, usually on a background of poorly controlled T2DM while receiving oral hypoglycaemic agents (OHAs). Management of hypoglycaemia, particularly when insulin is up titrated, will also be discussed. Further, we will look into intensifying insulin regimen when glycaemic targets are not achieved with a single injection of basal insulin. We will also explore when we need to stop further up titration, and refer to endocrinologists for secondary care. We hope that this article provides a pragmatic overview on the use of the insulin preparations commonly available in our primary care settings, and outlines the merits and disadvantages of these regimens. We will also make suggestions to help PCPs navigate through common clinical dilemmas with insulin, and encourage them to take a more proactive role in adopting insulin in primary care. Case 1Patient A is a 59-year-old lady with a history of T2DM for 8 years. She has a family history of diabetes with both father and older brother suffering from the disease. She is asymptomatic, and is compliant with the dietary and exercise advice you offered. Her oral drug regimen was gradually stepped up over the years, and now includes metformin 1g bd, gliclazide 160mg bd, and sitagliptin 100mg daily. She weighs 72kg with body mass index (BMI) 28.5 kg/ m2. Her latest eye examination showed mild nonproliferative diabetic retinopathy. Her latest blood results showed very high fasting glucose 10.5mmol/L and HbA1c 8.5%. She performs regular self-monitoring of blood glucose (SMBG) checks with the latest as follows.

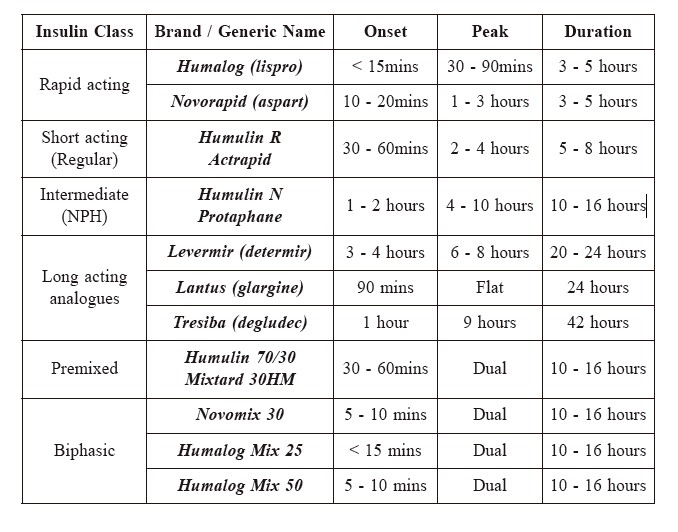
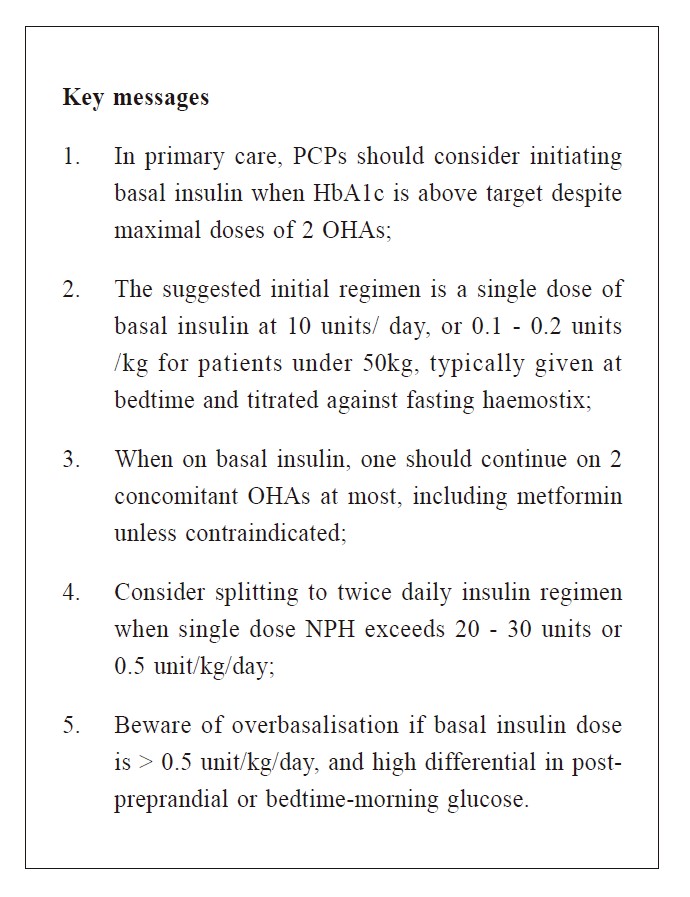
Scenario 1. When to initiate insulin in primary careWhile there is no unequivocal answer to when insulin must be initiated, it is well established that early intensive glycaemic control leads to persisting reduction in T2DM complications. It is therefore imperative for PCPs to overcome any therapeutic inertia towards insulin initiation, and recommend insulin treatment without delay when additions of more OHAs would unlikely bring about further therapeutic benefits. In primary care, the most common indication for insulin is when HbA1c is above glycaemic target despite maximal doses of OHAs. For example, the American Diabetes Association (ADA) recommends initiation of basal insulin when HbA1c remains uncontrolled after 3 months of triple combination of OHAs.1 Locally, it is suggested that insulin treatment should be considered when individualised targets were not met despite maximal doses of two or more OHAs.2 Early introduction of insulin should be considered if there is evidence of ongoing catabolism such as weight loss, symptoms of hyperglycaemia, or when glycaemic control is very poor (HbA1c > 10%, fasting blood glucose (FBG) ≥ 13.9 mmol/L, or random blood glucose (RBG) ≥ 16.7 mmol/L). Insulin is also indicated in acute decompensated conditions such as sepsis, acute myocardial infarction, hypoglycaemic hyperosmolar coma, or diabetic ketoacidosis (DKA), or when there is difficulty distinguishing the types of diabetes (Type 1 versus Type 2).1 There is no absolute contraindication for insulin, practicality, psychosocial circumstances, and patients’ acceptance should be taken into account. T2DM patients who have limited physical or cognitive capacity and thus are unable to self-manage insulin safely, and those with short life expectancy, may not be suitable for insulin. Likewise, patients who are poorly compliant to medications or SMBG, should not be started on insulin. Injection site pain, weight gain, and hypoglycaemia are the common unwanted effects of insulin therapy. All patients should be properly counselled by medical staff before the start of insulin treatment - information such as meal planning, exercise, SMBG targets, hypoglycaemia recognition and management, sick day plans, injection technique, and site rotation should be offered. Insulin-injection PreparationsInsulin preparations can be grossly classified as “basal” (i.e. intermediate and long-acting analogues) and “prandial” (ie. short and rapid acting analogues). Premixed insulins and biphasic analogues compose of both basal and prandial components. Different insulin preparations differ mainly in their time to action and their duration of action. Common insulin preparations, their onsets, peaks and durations of action are summarised in Table 1. Table 1: Common insulin preparations, their onsets, peaks and durations of action
Back, to our case, Patient A would be a prime candidate for insulin therapy as she is already on 3 classes of OHAs at maximal doses. Her latest HbA1c of 8.5% should serve as a call to action to change or intensify therapy, including initiation of insulin.
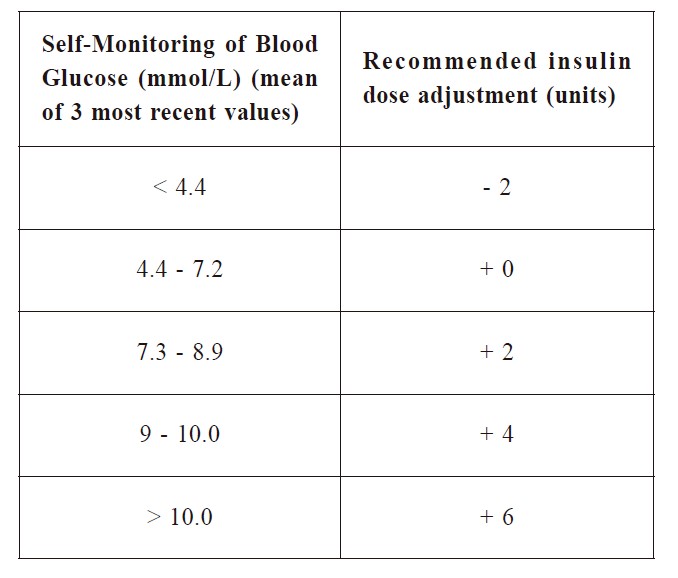
Scenario 2. How to initiate insulin in primary careA single daily dose of basal insulin, either NPH or detemir given at bedtime, or glargine or degludec given in the morning or at bedtime, is a reasonable initial regimen. The initial dose is usually 10 units or 0.1 - 0.2 unit/kg/day suggested by ADA guideline.1 The American Association of Clinical Endocrinologists (AACE), on the other hand, suggests initiating basal insulin on the basis of HbA1c levels: the total daily dose (TDD) of basal insulin is 0.1 – 0.2 unit/kg/day for HbA1c < 8%, and TDD of 0.2 – 0.3 unit/kg/day for HbA1c > 8%.3 Locally, we recommend a single dose of basal insulin at 10 units/day, or 0.1 - 0.2 unit/kg for patients under 50kg, typically given at bedtime. The first target after insulin initiation is to achieve optimal FBG levels (4.4 - 7.2 mmol/L). Patients should thus be instructed to test their fasting haemostix regularly, with occasional SMBG checks at various times the rest of the day. Titration should ideally commence within 2 weeks of insulin initiation, using this 2-week window as an opportunity to assess patient’s acceptance and familiarisation. Most algorithms in clinical trials suggest titrating basal insulin in small increments at short intervals, generally reaching steady state in 8 - 12 weeks. Outside of clinical trials, a more gradual schedule of adjustments, dependent on available resources, may be appropriate to facilitate monitoring and minimise hypoglycaemia. For persistent fasting hyperglycaemia, two approaches are recommended for titration of insulin dose. One is the physician-led approach (fast schedule), where insulin dose of 2 - 6 units is increased based on FBG level over the previous 2 - 3 days, and adjusted twice per week until FBG is < 6 mmol/L (Table 2). The other approach is the patient-led approach (slow schedule), where 2 units of insulin is increased every 3 days until FBG is in range (< 6 mmol/L). For either approach, insulin dose should only be increased when FBG is > 4 mmol/L. It is important to note that only approximately half of patients can achieve HbA1c ≤ 7% with insulin doses in the range of 40 - 70 unit/day.4 It is therefore sensible to emphasise to patients that their starting insulin dose is not likely to be the end dose, and gradual up titration should be expected.
Table 2: Titration of Insulin according to SMBG
A review of the concomitant OHAs use is always advisable. It is suggested that one should keep two OHAs at most, including metformin unless contraindicated.2 Metformin, when used in combination with insulin, is associated with better glycaemic control, fewer hypoglycaemic events, and less weight gain than with insulin alone.5 Generally speaking, sodium-glucose cotransporter 2 inhibitors (SGLT2i) or dipeptidyl peptidase-4 inhibitors (DPP4i) should be continued, as they exert synergistic effects with insulin to allow insulin dose to be reduced by up to 50% and confer minimal risks of hypoglycaemia. Reducing or discontinuing sulfonylureas on initiation of insulin should be considered, especially for those at higher risk of hypoglycaemia. Use of glitazones in combination with insulin is controversial, for although glitazones allow lower daily insulin requirements, they are associated with weight gain, fluid retention and congestive heart failure. Supramaximal doses of any OHAs should be reduced to the recommended maximum dose (i.e. metformin to no more than 2000mg per day). It may be worthwhile to inform patients that when discontinuing any OHAs, glucose rebound is expected, and this should not be misinterpreted as a failure of insulin therapy. Case 2Patient B is a 65-year-old gentleman with a 10-year history of T2DM. He was initiated on protaphane 10 units at bedtime 6 months ago, and the dose was up titrated over the next few months to 20 units with the support from the clinic diabetic nurses. He achieved a fasting haemostix of 6.0 mmol/L and HbA1c of 7.9 %. His concomitant OHAs were metformin 1 bd and dapagliflozin 10mg daily. However, Patient B reported experiencing several episodes of night time hypoglycaemia over the past month, which presented as sweating and palpitation that woke him up from sleep. These hypoglycaemic episodes were evident when you examine his SMBG logbook.

Scenario 3. How to manage frequent hypoglycaemia when on basal insulinIncreased incidence of iatrogenic hypoglycaemia is a by-product of intensive glucose lowering therapy, and is often the limiting factor in T2DM management. The risk of hypoglycaemia among T2DM patients new on insulin therapy is low, but increases with longer history of diabetes and duration of insulin treatment, warranting more vigilance from PCPs as the disease advances.6 Patients and their carers need to be educated on the management of hypoglycaemic episodes. The presence of any nocturnal hypoglycaemic symptoms, or low haemostix by SMBG, should alert PCPs to refrain from further insulin up titration. Underlying causes of hypoglycaemia should be sought - insufficient carbohydrate intake, irregular meal times, or unaccustomed exercises are common culprits. The dose of sulphonylureas should be reviewed. If no clear reason for hypoglycaemia is identified, insulin dose should be decreased by 4 units or 10 - 20%.1 Sensible option for Patient B, if no identifiable cause is found, is to switch his NPH to a long-acting insulin analogue. These analogues are particularly useful for avoiding nocturnal hypoglycaemia due to their peakless property. A unit-to-unit conversion of TDD from once daily NPH to long-acting analogues should suffice. If switching from twice daily NPH to once daily long-acting analogues, the recommended dose is 80% of the TDD NPH, to lower the risk of hypoglycaemia.7 Therefore, Patient B was advised to switch his protaphane before bedtime to degludec 20 units in the morning after discussion with his attending doctor, and his glycaemic control gradually improved without further episodes of nocturnal hypoglycaemia. Case 3Patient C is a 67-year-old gentleman and has been on protaphane for 8 months, along with his usual OHAs that include metformin 1000mg bd, pioglitazone 30mg daily and empagliflozin 25mg daily. The dose of protaphane was gradually up titrated to currently at 30 units bedtime. The titration process was well tolerated and uneventful, thanks to the support from the diabetic nurses. In consultation with you today, he reported no hypoglycaemic symptom. He weighs 74kg, with BMI 26.0kg/m2. However, his latest HbA1c last week remained poor at 9.0% with a fasting glucose of 7.0 mmol/L. His recent SMBG profile is as follows:

Scenario 4. How to intensify basal insulin when glycaemic targets not reachedA substantial number of patients with T2DM will eventually fail to maintain glycaemic control with once daily basal insulin because of progressive decline in ß-cell function. Typically, when patients are on about 20 - 30 units of basal insulin or when TDD exceeds 0.5 unit/kg/day and still not reaching their glycaemic targets, more complex insulin regimens may be called for to intensify treatment.8 When FBG is under control but HbA1c is still above target, we should then look into problems with preprandial and postprandial hyperglycaemia. Common options at GOPC’s disposal include addition of a morning dose of basal insulin, or a switch to twice daily premixed insulin. The choice between these two options should be individualised based on the patients’ SMBG profiles while on once daily basal insulin. An addition of a morning dose of basal insulin is effective to control pre-dinner hyperglycaemia. If pre-dinner haemostix is > 7.0 mmol/L, we may consider adding 4 units of basal insulin (except glargine and ultra-long analogues degludec) before breakfast on top of the usual bedtime basal insulin. While on twice daily basal insulin, patients should be instructed to monitor their fasting and pre-dinner haemostix, and insulin dose should be titrated accordingly. Twice daily premixed insulin may be more preferable if there is a need for postprandial coverage, and can be given pre-breakfast and pre-dinner. The prebreakfast dose of premixed insulin should be titrated according to pre-dinner haemostix, and the pre-dinner dose should be adjusted according to fasting haemostix. Patient C’s fasting blood glucose levels are near target, but his HbA1c remains elevated. We can note from his SMBG profile that his daytime glucose profile is persistently high with prominent postprandial surges. In this context, a switch to twice daily premixed insulin is favoured. This can be converted from unit to unit at the same TDD, with two third of that given in the morning and one third given at bedtime, or half am and half pm. We can increase dose by 1 - 2 units or 10 - 15% once or twice weekly until SMBG target is reached.9
Scenario 5. Efforts to avoid overbasalisationIt is important to recognise that while there are no upper limits to insulin dosage, there is a point at which further increase in basal insulin is no longer addressing glycaemic needs. This may occur when TDD of basal insulin is at 0.5 - 1.0 unit/kg, and may be an indication to stop further up titration. Overbasalisation occurs if over-aggressive effort is attempted to attain postprandial targets with basal insulin. Since basal insulin is not designed for postprandial coverage, overbasalisation may lead to hypoglycaemia in fasting states, without seeing additional reduction in HbA1c. Irregular meal times and increased physical activities can predispose patients to hypoglycaemia if too much basal insulin is given. Overbasalisation is associated with increased mortality, increased medical cost from hospitalisation, and impact on patient future compliance to therapy. Clinical cues that suggest overbasalisation include: (1) basal insulin dose is > 0.5 unit/kg/day; (2) high differential in post-preprandial glucose, or in bedtime (Be) - morning (AM) glucose: a BeAM value > 2.5 - 3.0 mmol/L signifies potential overbasalisation; (3) erratic hypoglycaemia during the day not tied to change in physical activity or meal alteration; and (4) high glycaemic variability.9 Presence of overbasalisation should prompt re-evaluation to further individualised therapy, and to ensure that patients monitor their SMBG at different times of the day.
Scenario 6. Sick day management for patients on insulin treatment in ambulatory settingsIntercurrent illnesses may precipitate severe manifestations of diabetes, so sick day management is directed towards preventing dehydration, hypoglycaemia and DKA. Patients are reminded to hydrate by drinking 125 - 250 ml of water every hour, and to never discontinue their insulin unless advised by a medical staff. More frequent blood glucose monitoring is recommended during episodes of illness. SMBG should be monitored at least 4 hourly, and more frequently as necessary if < 5 mmol/L or > 14 mmol/L. If patients have decreased oral intake and haemostix are in the low normal ranges, TDD of insulin may be decreased by one third. If hyperglycaemia >14 mmol/L develops, patients are advised to check urinary ketones with home testing. In the presence of urine ketones, vomiting, symptoms of DKA, or not tolerating any oral intake with haemostix < 4 mmol/L, hospital care should be sought. There should also be a low threshold for sulfonylureas and SGLT2i to be discontinued if patients are unable to eat and maintain hydration. In very mild illnesses where patients are able to eat close to their usual diet, they are encouraged to continue their usual diabetic regimen, including the use of insulin.10
Scenario 7. When to refer to an endocrinologist?PCPs may consider referring T2DM patients to specialists whenever they feel that further management is beyond their knowledge, resources and experiences. Common clinical scenarios that call for referral include frequent hypoglycaemia that limits further up titration, fluctuating glycaemic profile after initiating insulin for over 6 month, very high HbA1c (> 9.5%) despite on insulin for over 1 year, a TDD of insulin > 1 unit/kg/day, and patients requiring more complex insulin regimen.
When twice daily premixed insulin still fails to reach patients' individualised glycaemic targets, one may consider more advanced insulin regimens, such as addition of 4 - 5 units of rapid acting insulin, or 10% TDD of NPH dose, to the largest meal on top of basal insulin (basal plus therapy). Other injectable therapies such as Glucagon-like peptide-1 receptor agonists (GLP1 RA) are also viable options to address prandial hyperglycaemia. In the context of these novel agents, it would be reasonable to seek specialists’ opinion with regard to the most appropriate treatment.
ConclusionInitiation and titration of insulin therapy in T2DM patients can be simple and safe in the primary care settings by adopting a systematic approach. Timely introduction of insulin should be considered for T2DM patients whose HbA1c is persistently high (> 7.0%) after treatment on two or more OHAs. The preferred regimen for insulin initiation in most patients is once daily basal insulin at bedtime, and this should be titrated against morning fasting SMBG. Concomitant OHAs should be reviewed, keeping no more than two OHAs with the use of insulin. Long-acting insulin analogues should be considered if patients experience recurrent hypoglycaemia on NPH treatment. When glycaemic targets are not attained despite basal NPH insulin of > 30 units, or when further titration is limited by hypoglycaemia, insulin regimen should be intensified by the addition of a morning dose of NPH, or a switch to twice daily premixed insulins according to SMBG profiles and patients’ preference. References
Derek GC Ying,
LMCHK, FHKAM (Family Medicine), FHKCFP, FRACGP
Catherine XR Chen,
LMCHK, FHKAM (Family Medicine), PhD (Med, HKU), MRCP (UK)
Correspondence to:
Dr. Derek GC Ying, Room 622, 6/F, Nursing Quartar,
|
|