
|
September 2024,Volume 46, No.3
|
Original Article
|
Automated office waiting-area blood pressure as a practical method to eliminate white coat effect in conventional office blood pressure measurement in Chinese older people in a clinic setting in Hong KongShu-piu Leung 梁樹標 HK Pract 2024;46:53-59
SummaryObjective: To investigate whether automated office blood pressure measurement in the waiting area (wa- AOBP) can effectively eliminate the white coat effect (WCE) in blood pressure (BP) measurement and to evaluate the comparability of wa-AOBP and home blood pressure monitoring (HBPM) measurements.Design: A cross-sectional study. Subjects: 133 Chinese people aged 65 years or above attending a private general practice clinic. Main outcome measures: Conventional office blood pressure (COBP), wa-AOBP and HBPM Results: The systolic BP (SBP) for COBP, wa-AOBP and HBPM were 133.5 ± 13.2, 127.8 ± 11.0 and 126.2 ± 7.6 mmHg respectively. The diastolic BP (DBP) for COBP, wa-AOBP and HBPM were 73.3 ± 9.9, 70.9 ± 8.2 and 73.3 ± 7.3 mmHg respectively. The differences in SBP and DBP between COBP and wa-AOBP were 5.7 ± 7.8 mmHg, (p < 0.001) and 2.4 ± 5.2 mmHg (p < 0.001) respectively. The differences in SBP and DBP between HBPM and wa-AOBP were -1.4 ± 11.0 mmHg (p = 0.149) and 2.4 ± 7.3 mmHg (p < 0.001) respectively. Conclusions: Our study suggests that wa-AOBP is effective in the elimination of the WCE of COBP measurement for older people in a clinic setting, the effect of which is comparable with HBPM. Keywords: blood pressure measurement, automated office blood pressure, white coat effect, older people
摘要目的:探討診所等候區的自動化血壓測量(wa-AOBP) 是 否能夠有效消除白袍效應,以及評估wa-AOBP 與自我血 壓監測(HBPM) 的可比性。設計:橫斷面研究 對象:133 名65 歲或以上,在私家普通科診所就醫的華 人。 主要量度目標:傳統診所血壓測量 (COBP)、wa-AOBP 及 HBPM。 結果:COBP、wa-AOBP 及HBPM 的收縮壓分別為133.5 ± 13.2、127.8 ± 11.0及126.2 ± 7.6 mmHg,而舒張壓則分別 為73.3 ± 9.9、70.9 ± 8.2 及73.3 ± 7.3 mmHg。COBP 與wa- AOBP 之間的收縮壓及舒張壓差異分別為5.7 ± 7.8 mmHg (p < 0.001) 及2.4 ± 5.2 mmHg (p < 0.001)。HBPM 與wa- AOBP 之間的收縮壓及舒張壓差異則分別為 -1.4 ± 11.0 mmHg (p=0.149) 及2.4 ± 7.3 mmHg (p < 0.001)。 結論: 研究顯示wa-AOBP 能夠有效消除老年人在診所 環境中進行COBP 測量所產生的白袍效應, 其效果與 HBPM 相若。 關鍵詞:血壓測量,診所自動化血壓測量,白袍效應, 老年人 IntroductionBackgroundThe prevalence of hypertension (HT) in Hong Kong is 64.8% for people older than 65 years.1 The prevalence increases to 90% after 85 years of age.2 Optimal blood pressure (BP) control effectively reduces the risk of adverse cardiovascular (CV) events. The 2015 Systolic Blood Pressure Intervention Trial (SPRINT) concluded that among patients at high risk for CV events, a systolic blood pressure (SBP) of < 120 mmHg as measured by unattended office BP measurement, when compared to a SBP of < 140, was associated with a significantly lower rate of CV events.3 The 2017 American College of Cardiology / American Heart Association (ACC/AHA) guideline on the management of HT lowered the treatment target from 140/90 mmHg to 130/80 mmHg.4 Currently there is no consensus on the target BP for the treatment of HT in older people, but it is increasingly recognised that special considerations for target BP should be given to the management of older people with HT.5,6 The target BP should be relaxed according to the functional reserve and frailty levels. Chronological age should not be the only criterion for adapting therapeutic strategies because of the large heterogeneity in the ageing process among older people. The recommendations from most international guidelines make reference to BP measurements obtained by methods effective in eliminating the white coat effect (WCE). The condition refers to elevated BP measurements at clinics but normal by ambulatory blood pressure monitoring (ABPM) and/or home blood pressure monitoring (HBPM). WCE has been reported to over-estimate BP measurements by a mean of 9/7 mmHg.7 WCE is more common in older people and hence elimination of the WCE is especially important in this group.7,8 Overtreatment of HT based on over-estimated BP readings might result in increased risks of side-effects including malaise, dizziness, syncope and injurious falls.9 Conventional office blood pressure (COBP) has been the most widely used method of BP measurement in clinic settings. It is the BP measurement performed by a medical / healthcare professional, and provides BP readings within minutes for necessary medical action. However, even when a rest period of 5 minutes is allowed, COBP is still prone to inaccuracy due to the WCE.10 It is therefore important to identify more reliable methods of office BP measurement. Automated office blood pressure (AOBP) has been extensively studied as an alternative method of office BP measurement. It refers to repeated BP measurements unattended by medical professionals with the use of fully automated BP machines. AOBP has been shown to correlate more closely with daytime ABPM compared to COBP.11,12 The improved accuracy and precision of AOBP is attributed to its effective elimination of the WCE. Conventionally, AOBP measurement also requires the subject to be seated alone in a quiet consultation room. This arrangement, albeit an ideal setting to eliminate environmental effects on BP measurement, is not feasible in most clinic settings in Hong Kong due to insufficient consultation rooms, government and private clinics alike. Furthermore, it would be inappropriate to leave elderly patients in a clinic unattended for any length of time, as they are more prone to accidents and unexpected change of medical conditions. HBPM has been used as an alternative BP measurement method and has been shown to correlate closely with ABPM and effectively ameliorate the WCE.13 HBPM is, however, associated with reporter bias, and might not be feasible in older people with cognitive, neuromuscular or visual impairment. The current study considers a modification of the conventional AOBP by performing AOBP in the clinic waiting-area (wa-AOBP). The patient is seated in a corner of the clinic waiting area instead of in a single room for BP measurement, all conditions of the conventional AOBP measurement being otherwise retained. ObjectivesThe primary objective is to investigate whether wa-AOBP can effectively eliminate the WCE in blood pressure measurement. The secondary objective is to evaluate whether wa-AOBP and HBPM measurements are comparable. MethodsStudy DesignA cross-sectional cohort of Chinese older people attending a private out-patient clinic for the management of primary HT was recruited. All patients were referred from the government outpatient clinic (GOPC) under the GOPC public private partnership scheme. These patients had been followed up in the GOPC for at least one year and their BPs were considered stable before referral. Their co-morbid medical conditions were also considered to be under control. All Chinese subjects 65 years of age or older with primary HT and taking at least one anti-HT drug were included into the study. Subjects were excluded if they suffered from an intercurrent medical illness; if they required adjustment of anti-HT drug(s); if they were unable to perform BP measurement unattended; if they were not performing HBPM or if they were residing in old age homes at the time of recruitment. BP MeasurementUpon arrival at the clinic, the subject was arranged to sit at a corner of the waiting area. Procedures on COBP and wa-AOBP were explained by the research team and verbal consent obtained. The Omron HEM-907 automated BP machine was used. The machine had been validated for accuracy independent of the manufacturer in accordance with standard criteria.14 After a rest time of 5 minutes, COBP was measured and recorded by the clinic nurse. The subject was instructed not to move, talk or use the mobile phone during the BP measurement. The automatic mode of the BP machine was then activated, after which the nurse left and the subject was alone. Three wa-AOBP measurements were taken at one minute intervals starting 3 minutes after activation of the BP machine. The BP readings were hidden from the machine display during the whole procedure. The machine generated the average wa-AOBP reading which was then recorded. Consultation and Instructions for HBPMMedical consultation was conducted after the wa-AOBP measurements had been completed. Verbal consent was sought from the subjects to perform daytime HBPM. They were instructed to perform daily HBPM on the following 7 consecutive days in the same manner as they would normally do, and to record the readings on a chart provided to the subject. The subject was requested to return the chart to the clinic after completion. The subject would be reminded to complete the chart if he/ she failed to return the chart two weeks after the medical consultation. The mean of the seven daily BP measurements performed by the subject at home was used for data analysis. Statistical AnalysisSPSS statistical software (version 20) was used for data analysis. Descriptive statistics were used to summarise the data and continuous variables were reported as mean ± standard deviation (SD). Differences between BP readings by different BP measurement methods were computed and compared by paired sample t-test. Subgroup analysis on the difference between wa-AOBP and COBP readings was performed by independent 2-sample t-test. A difference of 5 mmHg or more between different BP measurement methods would be considered clinically significant. ResultsThe total number of patients attending the clinic for follow-up of HT during the study period from October 1 to December 31, 2019 was 299, among which 193 met the inclusion criteria (age > 65 years). 42 subjects were excluded for the following reasons: non-Chinese (2), presence of intercurrent illness (17), required adjustment of anti-HT drugs (4), no home BP machine (10), using wrist home BP machine (1), living in old age homes (1), moderate dementia / too frail (5) and planning on a trip (2). Among the 151 subjects recruited into the study, 133 completed the HBPM recording as arranged. The 18 subjects who failed to return the HBPM record initially either could not be contacted or refused to complete the record. The data on the remaining 133 subjects were analysed. The demographics of the subjects are shown in Table 1. Table 1: Demographics of the Study Subjects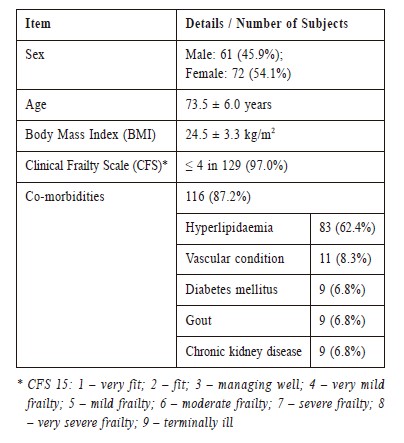
The SBP for COBP, wa-AOBP and HBPM were 133.5 ± 13.2, 127.8 ± 11.0 and 126.2 ± 7.6 mmHg respectively. The diastolic BP (DBP) for COBP, wa- AOBP and HBPM were 73.3 ± 9.9, 70.9 ± 8.2 and 73.3 ± 7.3 mmHg respectively. The differences in SBP and DBP between COBP vs. wa-AOBP, HBPM vs. wa- AOBP and COBP vs. HBPM are shown in Table 2. Table 2: Comparison of differences in BP readings between COBP, wa-AOBP and HBPM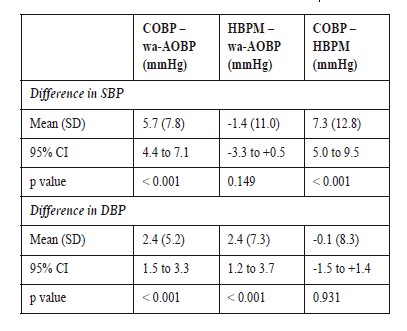
There was a statistically significant difference in SBP of -5.7 mmHg between COBP and wa-AOBP. The difference in SBP of -7.3 mmHg between COBP and HBPM was also significant. There was no statistical difference in SBP between HBPM and wa-AOBP. Although there were statistical differences in DBP between COBP vs. wa-AOBP and HBPM vs. wa-AOBP, they did not reach the pre-set clinically significant difference of 5 mmHg. Subgroup analysis on differences between wa-AOBP and COBP readings stratified according to age and SBP measurement by COBP was performed. There was no significant difference in SBP and DBP between the < 75 and ≥ 75 year age subgroups. Significant differences were noted in SBP and DBP between the SBP < 135 mmHg and ≥ 135 mmHg subgroups. The differences in SBP for the subjects in the lower and higher BP subgroups were -2.8 ± 7.8 mmHg and -9.3 ± 6.2 mmHg respectively (p < 0.001) and the differences in DBP for the lower and higher BP subgroups were -1.6 ± 5.4 mmHg and -3.4 ± 4.9 mmHg respectively (p = 0.05) Table 3. Table 3: Comparison of differences between wa-AOBP and COBP for different BP subgroups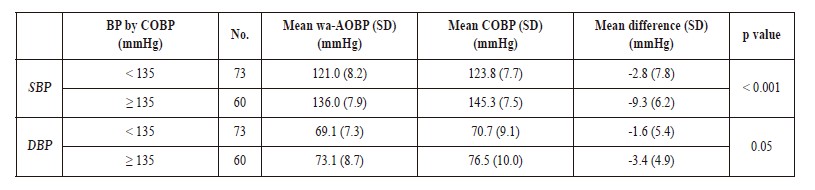
DiscussionOur study set out to identify a practically feasible method of office BP measurement. This is especially important for older people who might encounter difficulties in performing out-of-office BP measurements. COBP has long been known to correlate poorly with daytime ABPM because of the unavoidable WCE.10 Indeed, it has been suggested that COBP should be abandoned altogether.16 More recent data suggested that AOBP could eliminate most of the WCE, and hence should be adopted as the office BP measurement method.17 The 2018 ESH/ESC guideline and the 2017 Canadian hypertension guideline both recommend AOBP as the preferred method of BP measurement.18,19 The 2017 ACC/AHA guideline suggests that AOBP should be more widely used.4 The 2019 NICE guideline, however, refrains from making recommendations on the use of AOBP pending more conclusive research data.20 In the most recent systematic review and meta-analysis of 31 articles involving 9,279 participants comparing AOBP with daytime ABPM, readings were found to be similar, which suggested that AOBP did not exhibit the WCE associated with COBP.21 The study concluded that AOBP should replace COBP in the clinic setting. WCE has been hypothesised to be related to the presence of healthcare professionals during the BP measurement.22 There are two elements in conventional AOBP measurement that ameliorate the WCE: measurement with a fully automatic machine instead of being operated by a healthcare professional and being left alone quietly in a single room for more than two minutes.22 The latter is difficult to achieve in the local setting due to space constraints. If it can be demonstrated that being alone in a single room is not an essential element in eliminating the WCE during AOBP measurement, there is then a strong reason to adopt wa- AOBP as the routine method of office BP measurement. For the design of the procedure of BP measurement, we took both practical factors and the effectiveness of eliminating the WCE into consideration. In our study, we arranged the subject to be seated in a corner of the waiting area in a way that the clinic nurse would be out of sight of the subject as far as possible. We also started the first wa-AOBP measurement at 3 minutes so that any WCE would have resolved. The monitor display of the BP machine was deliberately hidden during the whole procedure so that any psychological impact of the BP reading on the subject would be avoided. Previous studies adopted a 2-minute interval between BP measurements, but available data showed that 1-minute interval gave similar results.23 In our study we hence adopted a 1-minute interval so that the duration of the procedure can be shortened. Previous studies adopted an average of 5 to 6 BP readings as the standard. Study data had since then shown that an average of 2 to 3 readings gave a similar result if a 5-minute rest time is allowed before the procedure.23 We hence adopted an average of 3 readings in our study. The whole procedure of wa-AOBP in our study hence involved a 5-minute rest time, a 3-minute flush time and two 1-minute waiting time between BP measurements. Considering the time for one BP measurement to be around 20 seconds, the whole procedure of wa-AOBP measurement in our study took 11 minutes. In real-life clinic practice, wa-AOBP measurement can start after a 5-minute rest time, and the whole procedure would take 8 minutes. This is not much longer than a properly performed COBP, when a 5-minute rest time would also be recommended before the BP measurement. We considered that a difference between methods of BP measurements would be clinically significant only if the BP readings were 5 mmHg or more. For a difference of less than 5 mmHg, it would be unlikely that any change in the clinical management including the adjustment of anti-HT drug dosage would be necessary. Our data showed a significant decrease in the mean wa-AOBP of 5.7/2.4 mmHg when compared with COBP. This indicated that wa-AOBP was an effective way to eliminate the WCE. The CAMBO trial demonstrated a greater decrease in the mean AOBP of 14/4 mmHg when compared to COBP taken during a previous visit.17 In the CAMBO trial, a manual manometric sphygmomanometer was used for COBP measurement in contrast to the electronic BP machine used in our study. This would have significantly reduced manipulation during inflation of the cuff and avoided the need for auscultation of the Korotkoff sounds during the BP measurement. Also, a rest time of 5 minutes was allowed before COBP measurement in our study, which was not a requirement in the CAMBO trial. These two differences might have accounted for the significantly lower COBP readings in our study, and hence a smaller difference. A third difference lies in the lower mean COBP in our study (133.5 ± 13.2 / 80.2 ± 9.9 mmHg) when compared to the CAMBO trial (149.5 ± 10.7 / 81.4 ± 8.5 mmHg). We demonstrated a significantly greater difference between COBP and wa-AOBP in the higher BP subgroup. The higher mean BP of the subjects in the CAMBO trial might have hence also contributed to the greater difference. When our wa-AOBP and HBPM data were compared, there was no significant difference in SBP while the difference in DBP was clinically nonsignificant. HBPM results also showed a significant decrease in SBP of 7.3 mmHg when compared with COBP. This is in agreement with other studies in which the difference was contributed to by the elimination of the WCE during HBPM measurement.13 Our results suggest that wa-AOBP effectively minimises the impact of WCE. Subgroup analysis was performed to identify characteristics associated with a greater difference between wa-AOBP and COBP, in which case the particular subgroup would benefit more from adopting wa-AOBP as the method of BP measurement. It is known that older people are more susceptible to the WCE.24,25 Our results, however, did not show any significant difference between the < 75 and the ≥ 75 year age groups, possibly due to the small sample size. When the lower SBP (< 135 mmHg) and the higher SBP (≥ 135 mmHg) groups were compared, there were significant differences in SBP of 6.5 mmHg and DBP of 1.8 mmHg. This indicates that the WCE is more marked in patients presenting to the clinic with a higher BP. This finding is practically important because under situations of constraint in resources, wa-AOBP can be reserved for the group of patients with sub-optimal BP control. Alternatively, wa-AOBP can be used for more reliable BP assessment when initial COBP measurement yields abnormally high BP readings. 
ConclusionOur results supported the hypothesis that wa-AOBP, like conventional AOBP, can effectively eliminate the WCE of COBP measurement. In contrast to COBP, wa-AOBP is performed in the absence of medical professionals by a fully automatic machine that provides automatic trigger and repeated measurements. All three elements contributed to the amelioration of the WCE during the BP measurement. Our data also supported the hypothesis that wa-AOBP and HBPM measurements are comparable. By obviating the need to occupy a single room during the BP measurement, wa-AOBP is a practical solution to a reliable office BP measurement method in most clinics in Hong Kong. The extra three minutes required for wa-AOBP measurement when compared to a standard COBP measurement should incur no significant extra burden to the running of a busy clinic. Although our results showed that the performance of wa-AOBP and HBPM were comparable, we do not propose to consider wa-AOBP as a substitute for HBPM. During HBPM, the patient takes an active role in the BP measurement, and as such, would enhance patient empowerment, reinforcement in life-style management and improvement in drug compliance.26 The roles of wa-AOBP and HBPM are hence complementary. ABPM is both resource and manpower demanding, and is best reserved for the more difficult situations. There are several limitations in our study. As we included subjects with relatively stable BP and the study was conducted in a clinic setting, the conclusions drawn from the study might not apply to diagnosis, subjects with extremes of BP and different medical settings such as old age homes and emergency departments. In our study, wa-AOBP was always performed after COBP. The results were hence susceptible to systematic order bias. In our study, there was no direct comparison of wa-AOBP against ABPM, the gold-standard of BP measurement. Further studies to establish the extent of elimination of the WCE would be necessary before wa-AOBP can be more widely adopted in clinical practice. It is best to conduct a direct comparative study between wa-AOBP and daytime ABPM. Alternatively, comparative study between wa-AOBP and conventional AOBP can be considered. FundingThe author did not receive funding for the current study. Conflicts of interestThe author has no conflicts of interest to declare. AcknowledgementThis study was conducted as part of the assessment for the degree of Master of Science in Gerontology at the Chinese University of Hong Kong. References
Leung Shu Piu,
MBBS (HK), FRCP (Edinburgh, Ireland), MSc Gerontology (CUHK)
Correspondence to: Dr. Shu-piu Leung, Shop 11, 1-7 Wu Kwong Street, Hunghom,
|
|