
|
June 2025,Volume 47, No.2
|
Discussion Paper
|
Managing patients with loneliness: A family physician’s perspectiveYuk-ting Tong 唐毓婷, Ting-kwan Li 李婷琨, Wai-man Yeung 楊偉民 HK Pract 2025;47:50-57 SummaryAs an emerging pervasive public health concern, loneliness has profound impacts on the physical and mental well-being of patients. This paper discusses the multifaceted risk factors that may predispose patients to loneliness, the detrimental health consequences it may bring, as well as the possible strategies we can adopt to mitigate loneliness. In addition, this paper also hopes to explore the potential role of family physicians in helping patients with loneliness. 摘要孤獨感作為一種新興的、普遍存在的公共衛生問題,對患者的身心健康有著深遠的影響。本文探討了可能導致患者產生孤獨感的多重風險因素、孤獨感可能帶來的有害健康後果,以及我們可以採取的緩解孤獨感的策略。此外,本文也希望探索家庭醫生在幫助孤獨患者方面的潛在作用。 IntroductionLoneliness has been a growing social concern both worldwide and locally, especially in the past few years as the COVID-19 pandemic brought about quarantine measures and social isolation which may have exacerbated loneliness. The World Health Organization (WHO) estimates that one in four older adults experience social isolation and 5% to 15% of adolescents suffer from loneliness worldwide.1 In Hong Kong, there are limited academic papers on the local epidemiology of loneliness. Nonetheless, various media and organisations have conducted surveys regarding loneliness. The Chinese University of Hong Kong (CUHK) and CUHK Jockey Club Institute of Aging found that 54% of adults aged 50 and above in Hong Kong experienced some degree of loneliness.2 A survey from The University of Hong Kong also revealed that nearly 60% of elderly aged 65 or above in Hong Kong experienced severe loneliness.3 The younger population also experience loneliness, as evidenced by a study conducted by the Hong Kong Federation of Youth Groups, which revealed that 47% of adolescents and young adults in Hong Kong aged 12 to 24 felt lonely.4 A recent local press article in 2024 also revealed that the percentage of elderlies suffering from moderate or severe loneliness increased from 35.3% to 68.3% since 2018.5 As we can see, there is a substantial proportion of the population with loneliness. Loneliness is not just an emotion, but a serious health concern that is associated with increased risks of physical and mental morbidities as well as increased mortality6, which we will explore further in this paper. Hence, it is without a doubt that loneliness is a significant social and health problem that deserves our attention. To combat loneliness, a combined effort from multidisciplinary healthcare professionals is required. In particular, as family physicians working in the community setting and seeing patients day in and day out, we have a deep understanding of the needs of individual patient and the community as a whole7, and should be more able to assist those patients suffering from loneliness. In this paper we will discuss the characteristics of loneliness including its definitions, risk factors, consequences and interventions. Moreover, we will offer some practical advice on how family physicians can help patients with loneliness in daily clinical practice. What is loneliness?There are various definitions of loneliness. The WHO8 defines loneliness as “the pain we feel when our social connections do not meet our needs”, whilst the United States Centers for Disease Control (CDC)6 defines loneliness as “the feeling of being alone, disconnected, or not close to others”. Loneliness is also described as a “negative emotional experience that results from a perceived or actual deficiency in one’s social relationships”.9 Moreover, loneliness can be temporary or chronic, and can vary in intensity during different periods.10 Even if one is socially surrounded by others, one can still feel lonely if a deeper connection with others is lacking. In fact, the European Commission has described this state with the “lack of meaningful relationship with a significant other or close friend” as emotional loneliness.10 It is important, however, to differentiate between being merely alone and loneliness. Being alone is simply a physical phenomenon when one is not around other people. One may be alone and feel at peace, without feelings of isolation – this is described as solitude.11 So even if one is socially isolated, one may not feel lonely. Nonetheless, social isolation may contribute to the development of loneliness in some patients.8 In clinical practice, we can use questionnaires as tools to help us more objectively assess loneliness in our patients. There are a wide variety of questionnaires, some more comprehensive and others more efficient. In a busy clinic, the 6-item DeJong Gierveld loneliness scale (Box 1) and 3-item UCLA loneliness scale (Box 2) are short and effective ways for a brief initial assessment of the presence and severity of loneliness. For a more comprehensive assessment, the clinician may consider the full 11-item DeJong Gierveld loneliness scale and the 20-item UCLA loneliness scale.12 Box 1: 6-item DeJong Gierveld Loneliness scale13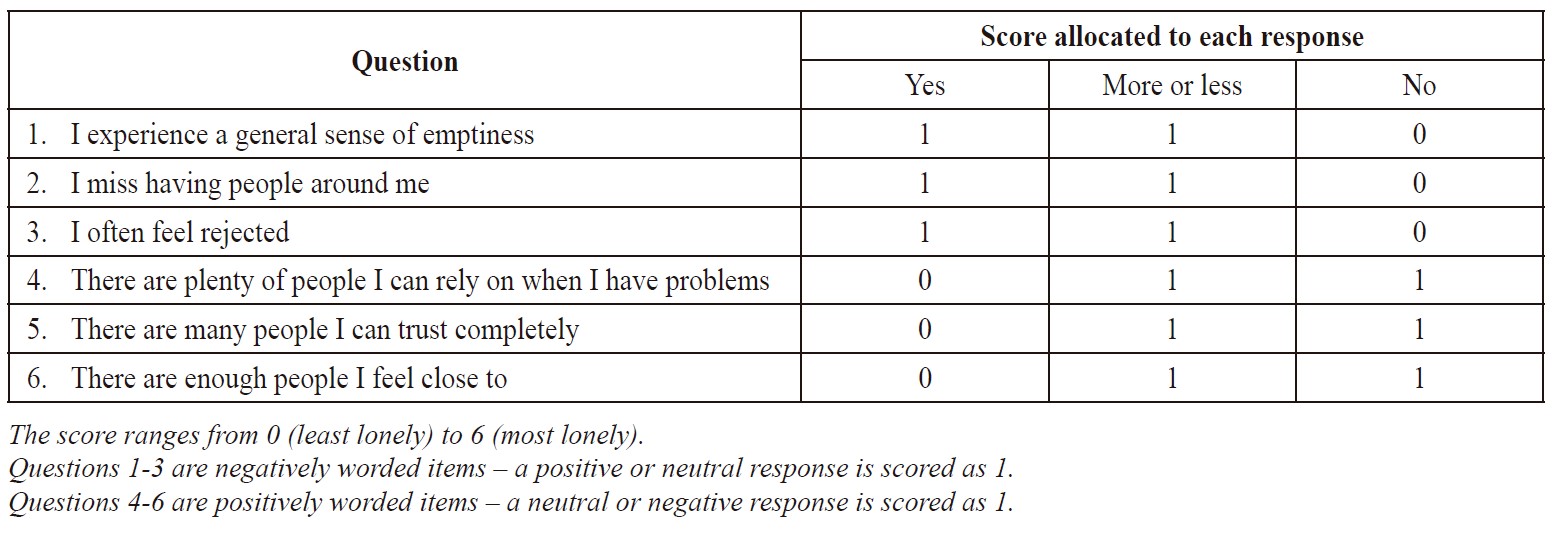
Box 2: UCLA 3-item loneliness scale14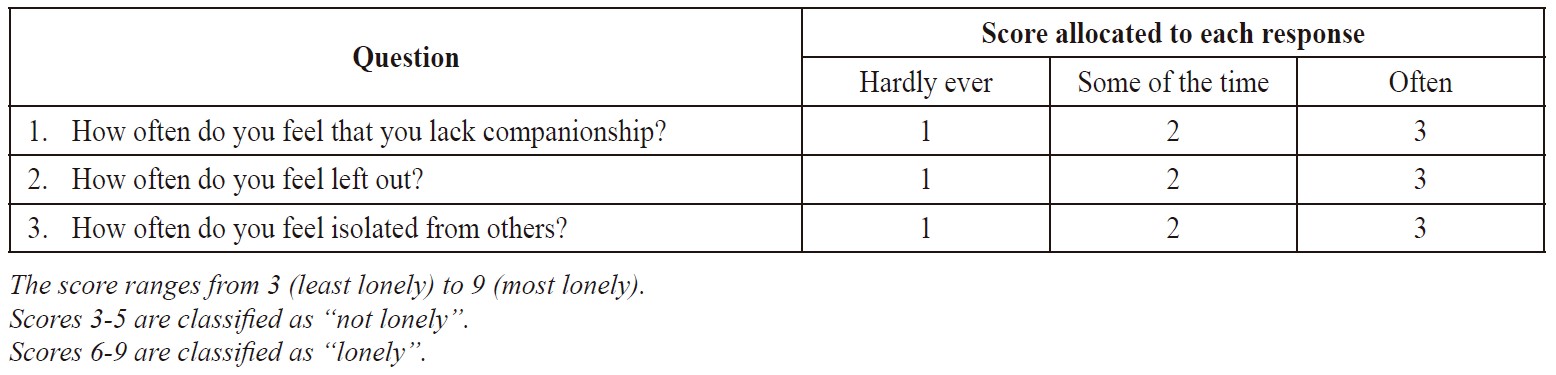
Patients with loneliness in real life practiceLoneliness is universal and can occur to anybody, anywhere, and at any time during one’s life or their family life cycle, be it in the stages of family founding, child bearing, child rearing (Case description 1), child launching, empty nest (Case description 2) or aging family (Case description 3). In particular, the empty nest syndrome is not an uncommon phenomenon in the family life cycle that is described as the ‘psychological conditions of unhappiness, anxiety, stress, worry, loneliness, and depression due to the children’s departure from the parental home’ and has been suggested to intensify loneliness.15 Below are some examples clinicians may encounter in their practice. Case description 1
James is a 32-year-old married engineer who has a one-year-old daughter. At the end of a consultation for his upper respiratory tract infection, he appears to be troubled by something. On further discussion, he expresses that he has been feeling increasingly disconnected from his wife ever since the birth of his daughter, as the majority of his wife's attention and care has been given to their child. He feels like he has lost the meaningful emotional connection with his wife and feels lonely. Case description 2
Mrs. Fung, a 56-year-old lady living with her husband, follows up with her family physician for hypertension. Her 24-year-old daughter has moved out recently, and she expresses having feelings of emptiness and loneliness ever since. Despite frequent communications on the phone with her daughter, she cannot help but experience the ‘empty nest syndrome’. Case description 3
Mrs. Chan, a 72-year-old lady who attends the doctor for a follow-up for her diabetes and hyperlipidaemia, had previously enjoyed a harmonious relationship with her 80-year-old husband. However, in the past two years, her husband has been showing signs of dementia and would sometimes forget who she is. She describes her husband as being “physically here but not mentally here anymore”. She feels like she is losing her partner in life, and she feels lonely and socially disconnected from the world around her. It is important to bear in mind that most patients may present to us with a physical chief complaint.16 However, the somatic reason for encounter may just be the tip of the iceberg, and there could be submerged a bigger underlying psychosocial problem such as loneliness, which the patient may not share unless we opportunistically screen for it.17 The authors believe there are multiple reasons for this. Firstly, loneliness is a state of mind, rather than an exact symptom, thus patients may not seek to explicitly voice it out. Secondly, it is an emotion, and, from a patient’s point of view, it may not be seen as a valid complaint with a potential treatment that can be offered. Thirdly, it can be embarrassing and deeply personal, thus many patients may choose not to share it. Given these reasons, it is likely that loneliness may be underrecognised. Hence, family physicians should maintain a high level of awareness and offer anticipatory care to those at risk of loneliness for prevention, and offer early assessment and prompt intervention to those already suffering from loneliness to minimise its complications. Table 1: Risk factors for loneliness18-24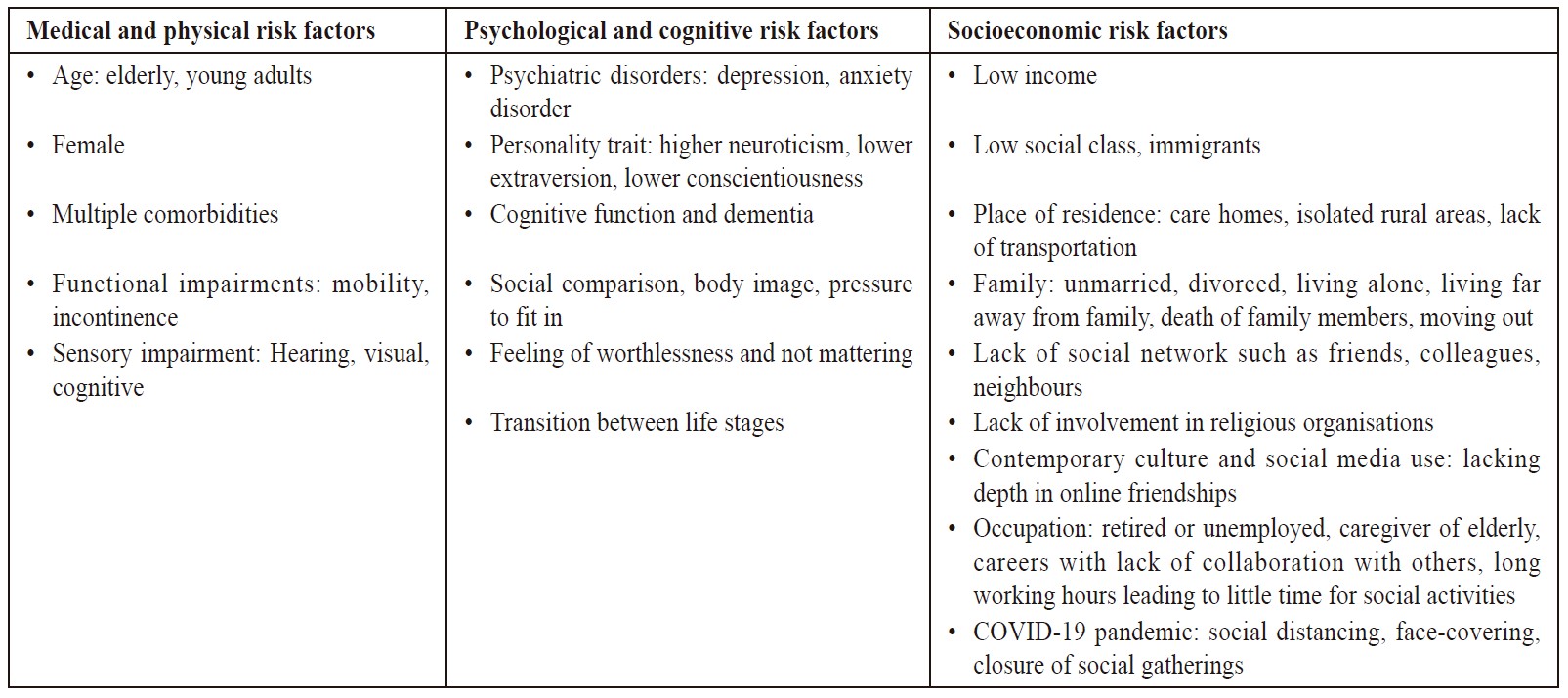
Which patients are at risk of developing loneliness?Several physical, psychological and socioeconomic factors have been reported to increase the risk of developing loneliness (Table 1). These factors can also interact with each other and further aggravate the risk. For example, an elderly living alone and with multiple medical comorbidities may not only have distress and difficulty in self-care as a result of her physical illnesses, but may also be more likely to be confined at home and be socially isolated, which can further contribute to the development of loneliness and other mood problems. Case description 4
Amy is a 78-year-old widowed lady who
has a past medical history of hypertension,
hyperlipidemia, congestive heart failure and
gout. She lives alone in a public housing estate.
She is able to walk with a stick but sometimes
finds it difficult to take care of household
chores by herself, especially when her mobility
is limited by lower limb oedema or gouty
attacks on her feet. She has a son who has now
emigrated overseas. Amy is financially tight and
is dependent on her old age allowance and the
occasional financial subsidy from her son.
What are the consequences of loneliness?A meta-analysis in 2015 showed that loneliness and social isolation were associated with an increased mortality risk of 26% and 29% respectively.18 This is comparable to smoking 15 cigarettes per day and having an alcohol use disorder.18 In addition, several other biological, psychological and behavioural health consequences of loneliness have also been reported (Table 2). These complications can further worsen the patient’s pre-existing conditions, which may concomitantly be risk factors for loneliness, thereby leading to a vicious cycle (Figure 1). Figure 1: The interrelationship between loneliness, its risk factors and its consequencesLoneliness may lead to various biological, psychosocial or behavioural consequences, either directly or indirectly, and those consequences may themselves be risk factors that aggravate loneliness 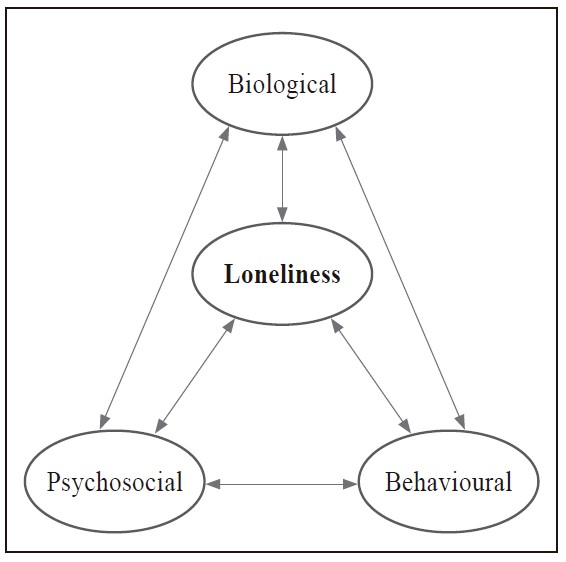
Table 2: Health consequences of loneliness18,19,25-27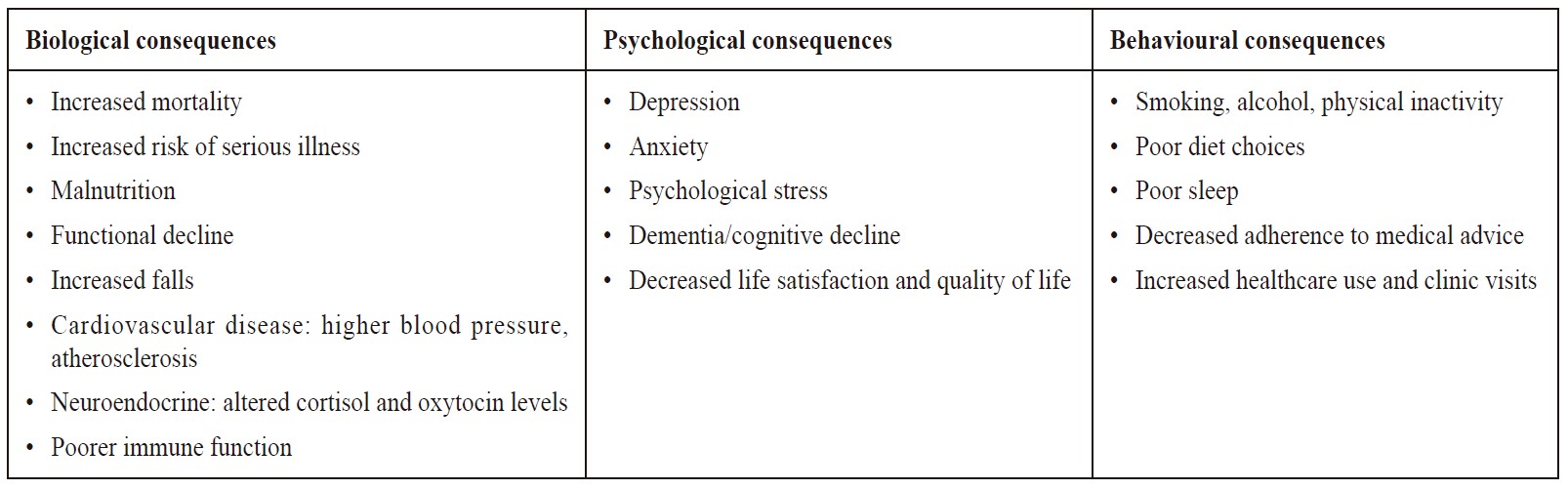
Loneliness and its negative feelings may, rather understandably, be associated with psychological consequences such as depression and anxiety. This stress may also play a role in behavioural modification such as physical inactivity, smoking and sleep disruption. Biologically, there have also been proposed mechanisms suggesting that loneliness and its chronic social stress may increase cytokine and pro-inflammatory monocytes production, which may potentiate glucocorticoid resistance, resulting in augmented inflammation and oxidative stress that may play a role in atherosclerosis development and blood pressure elevation. The definite causal relationship of loneliness with these consequences are, however, not yet well demonstrated, but its associations have been evident.28 What interventions can reduce loneliness?There are simple things that we can do to help those with loneliness, such as giving them empathy with active listening, and also encouraging family and friends to show support and keep in touch with them.29 We can also consider other specific interventions to reduce loneliness, examples of which have been listed in Table 3 . A literature review by the European Commission Joint Research Centre found that the interventions are generally effective, although the magnitude of the effectiveness varies across different intervention types and with different targeted population groups.30 Despite these known interventions, it can still be difficult to tackle the problem of loneliness in some patients. A patient-centred approach should be employed when selecting the intervention modalities, taking into account the patient’s preference, the patient’s physical condition and the feasibility of the intervention. Sometimes there may be barriers to implementing interventions. For example, in Amy’s case (Case description 4) , chronic illness such as heart failure and gout may limit a patient’s mobility, and sensory losses such as hearing impairment can restrict a patient’s communication and social engagement. Financial cost and transportation needs are other factors to consider when selecting interventions for our patients.18 Table 3: Specific interventions to reduce loneliness30-33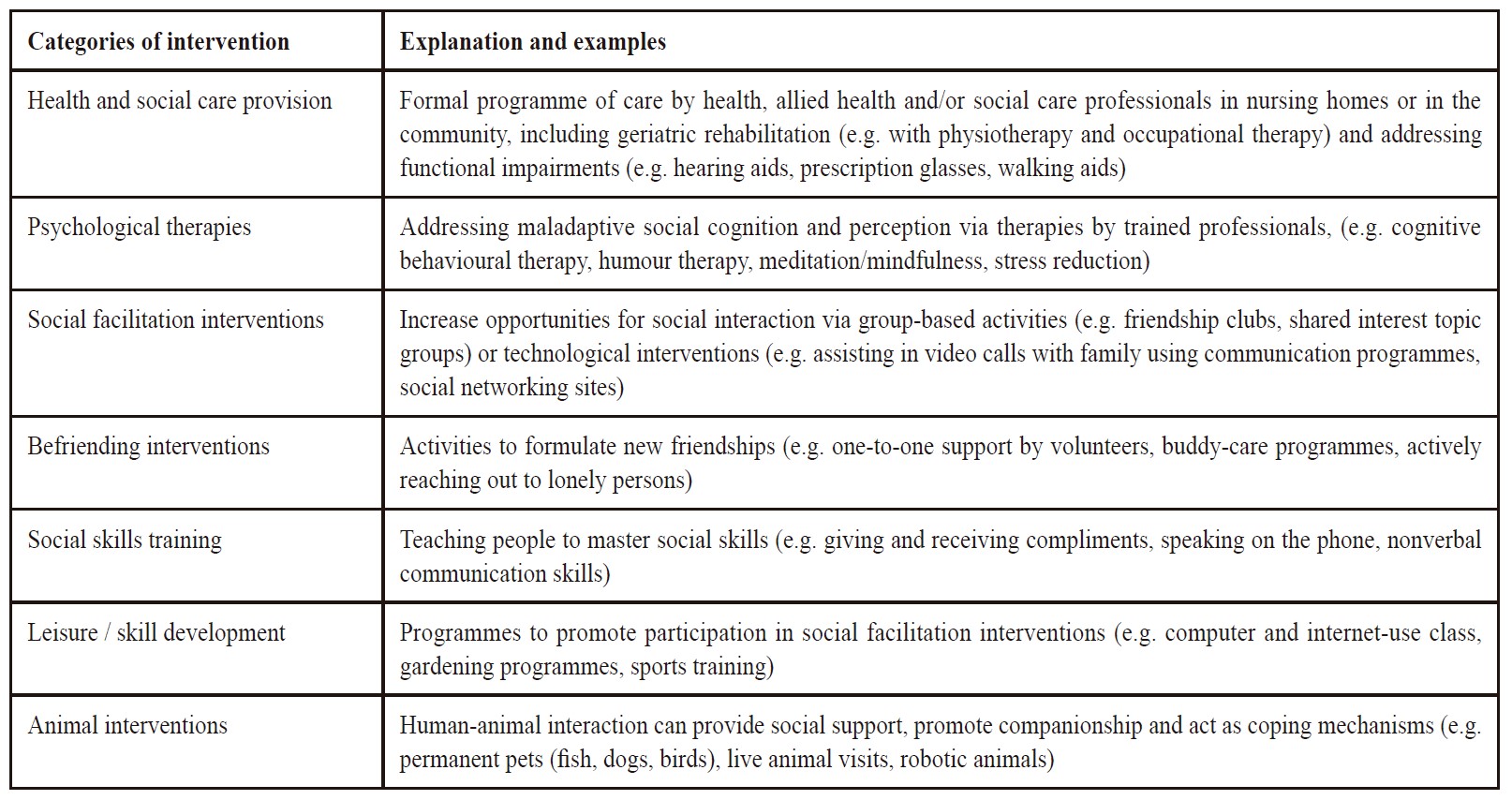
Hence, to reduce these barriers we can start with optimising Amy’s underlying physical conditions by prescribing medical treatment, utilising hearing aids to improve her sensory impairment and referring her to physiotherapists and occupational therapists for her mobility issues. For her mood condition, we can offer counselling, drug therapy and referral to a psychologist or psychiatrist for further management. We can then select specific interventions for reducing loneliness that are appropriate for Amy. Whilst physical activities may be less feasible for her, social facilitation such as interactive community programmes for the elderly and psychological therapies such as mindfulness may be employed. These interventions may take place in the community, and there are various resources for these purposes, such as elderly health centres. Last but not least, it is important to contact Amy’s relatives to explore their family relations and the potential support that they may offer. However, some relatives or caregivers may also have their own difficulties and underlying health issues, which may warrant the family physician’s further attention and assistance. Whilst the interventions mentioned above are useful in reducing loneliness, they may at the same time be useful strategies for preventing the development of loneliness in people who are at risk. HikikomoriWhilst social isolation may contribute to the development of loneliness8, loneliness likewise may intensify social isolation. Hikikomori is a term used to describe adolescents and young adults with a form of severe social withdrawal. A portion of cases of hikikomori may be classifiable with existing DSM (Diagnostic and Statistical Manual of Mental Disorders) criteria, but some do not meet the criteria for any existing psychiatric disorder, and hence there has been research exploring the possibility of the development of a DSM criterion for hikikomori.34 Whilst the term originates from Japan, Hikikomori is not uncommon in Hong Kong. A cross-sectional study from the International Journal of Social Psychiatry in 2015 estimates a prevalence of 1.9% to 2.6% of severe social withdrawal (hikikomori) in Hong Kong.35 Coupled with particular psychological beliefs and socioeconomic backgrounds which may make patients more maladaptive, these risk factors may predispose patients to social isolation and loneliness. Case description 5
A middle-aged lady comes to the doctor asking for advice about her son. She notices that her son, Kevin, aged 19, has become increasingly socially withdrawn. He rarely speaks to his family, and remains holed up in his room all day long – waking up late, then playing video games for the whole day with the occasional meal in between. He has not left the home for months and has dropped out from school since last year. Kevin’s mother is very worried, and upon doing some online research, she has come across the term ‘Hikikomori’ and wants to ask for the doctor’s expert opinion. Though many factors may contribute to hikikomori, such as the presence of other psychiatric disorders, loneliness has also been suggested to play a role.36,37 Loneliness does not just occur in older patients, but is also present in children and young adults. For cases of hikikomori or young adults with loneliness, such as Kevin, the reduced help-seeking behaviour may prove to be a barrier for identification and intervention.38 Hence, in these cases, the family would play an important role, be it in help-seeking (like Kevin’s mother) or in implementing interventions. Social facilitation interventions, especially those to improve family communication and bonding, may help adolescents with loneliness. Moreover, animalbased therapies may also be especially suitable for these young adults.39 A meta-analysis explicitly focusing on investigating the effectiveness of loneliness interventions on young people also supported the use of interventions such as social skills training, learning a new hobby, psychological therapy and enhancing social support for younger people.40 Key messages
DiscussionAs family physicians, we are in a unique position with the unparalleled advantage to prevent, identify, assess and intervene insidious epidemic health problems posing significant health consequences. As the initial points of contact, we are the first to identify patients who are at risk of or already suffering from loneliness, and our comprehensive and coordinating nature also allows us to provide a holistic and personalised care plan, extending beyond the chief reason for encounter. Moreover, it is not uncommon for us to be the sole family physician for the patient’s entire family. This special bond gives us a deeper insight into the patient’s household dynamics, and helps us facilitate the communication within the family to dampen the patient’s sense of loneliness. Admittedly, time constraint may be a limiting factor for us to fully explore and manage a patient’s loneliness in one single consultation, especially in a busy clinic setting. Fortunately, our solid rapport and continual relationship with the patient can help ameliorate this difficulty. As we are already familiar with the patient, we can astutely pick up our patient’s needs, and at the same time, we can continue to manage the patient’s loneliness through a series of subsequent follow-up visits. Given these characteristics, the authors feel that family physicians are well suited to help those with loneliness. It is evident from the above that loneliness is a prevalent health concern in our society. It may happen to anyone – be it the patient we saw this morning, the neighbour’s child going to school, the elderly on his way to buy groceries or the friend we bumped into yesterday. To tackle this societal problem, we need a collective effort from everyone. But as healthcare professionals, especially family physicians as specialists working in the community, we need to become leaders in coordinating these changes. Sometimes there may be limited strategies for us to alter the factors contributing to a patient’s physical state of being alone, but the caring attitude of family physicians may be therapeutic in itself. By giving realistic hope and implementing simple interventions such as educating mindfulness techniques, we may help patients lessen the sensation of loneliness. Developing positive thinking in those around us can create a multiplying synergistic effect in our society. Further public health surveillance interventions, health talks and exhibitions, medical conferences, communication between professionals and publications are all ways to help mitigate loneliness. Whilst there have been literature reviews showing positive effects of various interventions on loneliness, further research such as longitudinal studies on interventions on different population groups may be useful as the effectiveness of each intervention may ultimately be affected by various factors including the persons’ age, socio-cultural background and needs. It is not easy to combat loneliness, and we will need to collaborate with other professions to work hand in hand, but hopefully this paper will play a small role in tackling loneliness as a community health problem. References
Yuk-ting Tong,
MB ChB (CUHK)
Ting-kwan Li,
MB ChB (CUHK)
Wai-man Yeung,
MBBS(HK), FRCSEd, FRACGP, FHKAM (Family Medicine)
Correspondence to: Dr. Wai-man Yeung, Associate Consultant, Shau Kei Wan Jockey Club
|
|