
|
June 2025,Volume 47, No.2
|
Original Article
|
Barriers and facilitators to the implementation of telemedicine-based, real-time, online consultation among family physicians working in the public sector – a qualitative studyChi-yung Yan 殷志勇 HK Pract 2025;47: 32-40 Abstract
Background:
Teleconsultation (telemedicine-based, real-time,
online consultation) was adopted worldwide to offer
healthcare in response to the COVID-19 pandemic, but
this service was generally unavailable via the Hong Kong
public primary care system. Instead, medication refills
without consultations were offered to most patients.
Keywords: Teleconsultation, telemedicine, primary care, Family Physicians, Hong Kong
摘要
背景:為應對新型冠狀病毒感染大流行,世界各地應用遠程會診以提供醫療服務,然而這個服務在香港公營醫療環
境並不普及,取而代之的是免診取藥的方法。 關鍵詞:遠程會診、遠程醫療、基層醫療、家庭醫生、香港 IntroductionTeleconsultation is defined as telemedicinebased, real-time, online consultation between medical professionals and patients.1 It helps overcoming distance and increasing accessibility of healthcare in both developing and developed regions.2 However, its use in primary care was relatively limited before the COVID-19 pandemic.3 Under the COVID-19 crisis, teleconsultation has the advantage of maintaining healthcare access while preserving social isolation.4 The global use of teleconsultation has increased dramatically since the COVID-19 pandemic5,6, especially in primary care.6-8 A systematic review of teleconsultation in primary care services found that teleconsultations were non-inferior to face-to-face in-person consultations in improving clinical outcomes.9 In Hong Kong, in early 2020, when this research was planned, a significant number of medical appointments were cancelled or postponed due to the patients’ fear of COVID-19 infection and the infection control policy of healthcare providers.10 A local survey of residents aged 55 or above reported that 58.15% of respondents considered themselves to have a moderate or high risk of COVID-19 infection, and 61.3% said they were willing or very willing to try teleconsultation when relevant technology was fully developed.11 In response to this service need, increasing healthcare services in Hong Kong adopted teleconsultation. An ophthalmology unit utilising teleconsultation reported retaining 80% of outpatient services while maintaining social isolation.12 Teleconsultation in stroke clinics and geriatric psychiatry reported favourable responses with patients.13,14 Private primary care providers also15,16 started utilising teleconsultation. However, in the public primary care system, teleconsultation was generally not available. Instead, consultations were kept to a minimum, and medication was refilled without consultations for follow-up patients unless their conditions were unstable. This was a critical service gap, considering that the Hong Kong primary care services has an attendance of almost 6 million attendances per year.17 To implement teleconsultation among public Family Physicians, exploring factors affecting their readiness for teleconsultation is an essential step according to technology implementation models.18,19 Barriers and facilitators identified in foreign research revolved around workload, rapport with patients, user-friendliness, IT security and reliability, quality and safety of patient care, and organisational support related to teleconsultation.20-23 While foreign data may serve as a reference, local Family Physicians’ views are likely more relevant. Hong Kong’s local context24 in terms of our low doctor-to-patient ratio25, small geographical size, and aging population with a heavy chronic disease burden26 has to be considered. This study aimed to explore the barriers and facilitators to the implementation of teleconsultation perceived by Family Physicians in the public sector, in hopes to gauge their readiness and facilitate its smooth implementation.
Methods
Study DesignThis was a qualitative study based on individual semi-structured interviews. A qualitative design was a recognised method to investigate the barriers and facilitators perceived by participants during the implementation process.27 In addition, participants’ beliefs, values, and attitudes towards implementation of teleconsultation could be difficult to be quantified.28 Individual interviews with follow-up and probing questions could generate rich information.28 Family Physicians could give personal opinions about department policy without the peer pressure to be ‘politically correct’ in group interviews.29 It was important as the genuine facilitators and barriers perceived by staff were key to implementing teleconsultation.21
Setting and contextThis study was conducted from 8th February 2021 to 30th March 2021 when Hong Kong was combating the fourth wave of COVID-19. Family Physicians from the New Territories East Cluster (NTEC) under the Hospital Authority (HA) were recruited because they would be responsible for implementing a new service within their cluster. Cross-cluster opinions might not apply to each other due to different patient mix, service structures, resources, and management cultures.24 Participants from different General Outpatient Clinics and Family Medicine Centers within the cluster were recruited to ensure information collection was both diversified and generalisable to each facility.
Sampling strategyStratified purposive sampling was adopted to recruit Family Physicians including department heads, in-charge doctors of clinics, and frontline doctors since the implementation process was a team effort.27 Senior doctors who would potentially be responsible for making policy and supervising the implementation of teleconsultation, and frontline doctors who would potentially be responsible for conducting teleconsultation were purposively selected. A review of expert opinions recommended that the size of the purposive sample should be estimated inductively according to sample heterogenicity and purpose of the study30, and sampling should be continued until data saturation which was defined as no additional insights and new themes can be extracted from the participants.30 Although a comparison with similar qualitative studies21 suggested a sample size from 4 to 16, this study's final and adequate sample size would be known only when actual data saturation occurred.
Ethics approvalThe study was conducted according to the Declaration of Helsinki, with prior approval from the Joint Chinese University of Hong Kong – New Territories East Cluster Clinical Research Ethics Committee. Written consents were obtained from participants and no compensation was provided.
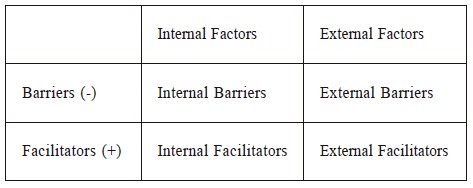
Development of Interview GuideA semi-structured interview guide was designed primarily to explore facilitators and barriers to implementing teleconsultation perceived by Family Physicians working in the public sector. It also explored Family Physicians’ experience and readiness for teleconsultation. Interview questions (Appendix A) were based on a literature search which showed that the factors affecting the implementation of telemedicine could be divided into facilitators and barriers.20,21,23,31 These facilitators and barriers could be internal or external (Table 1). ‘Internal’ refers to system users’ behaviour and motivation while using teleconsultation. ‘External’ refers to the teleconsultation system and the environment surrounding it, such as information infrastructure, medical-legal, and medical insurance support. The barriers and facilitators reported in the literature were also used in developing probes for the interview questions.20,21,23,31 The interview questions were field-tested and then refined with a pilot test as recommended by literature32, after interviewing 10% of the estimated sample size (i.e., 2 Family Physicians) as a general agreement.33 Table 1: The framework of factors affecting the implementation of teleconsultation
Data Collection and AnalysisIndividual face-to-face interviews were conducted in (Cantonese) Chinese. The process was audiotaped and transcribed in verbatim. The transcripts were returned to the participants to ensure accuracy. Thematic analysis was conducted on the transcripts by the framework of Braun and Clarke.34 Keywords and repeated phrases in the transcripts were organised into meaningful and conceptual codes by open coding first. Those codes were then grouped into subcategories by axial coding. Subcategories were then summarised into themes. Important quotes were reported in the result section to illustrate the themes and allow readers to assess consistency between the data and the interpretation.35
ResultsData saturation was achieved after interviewing 15 Family Physicians. Their background characteristics were summarised in Table 2. Characteristics of each participant were listed in Table 3. 2 participants (13%) reported experience as teleconsultation providers. 2 participants (13%) reported experience as teleconsultation users. 5 participants (33%) reported learning experience with teleconsultation in the forms of group discussion, conferences, or seminars. Table 2: Summary of participantsʼ characteristics
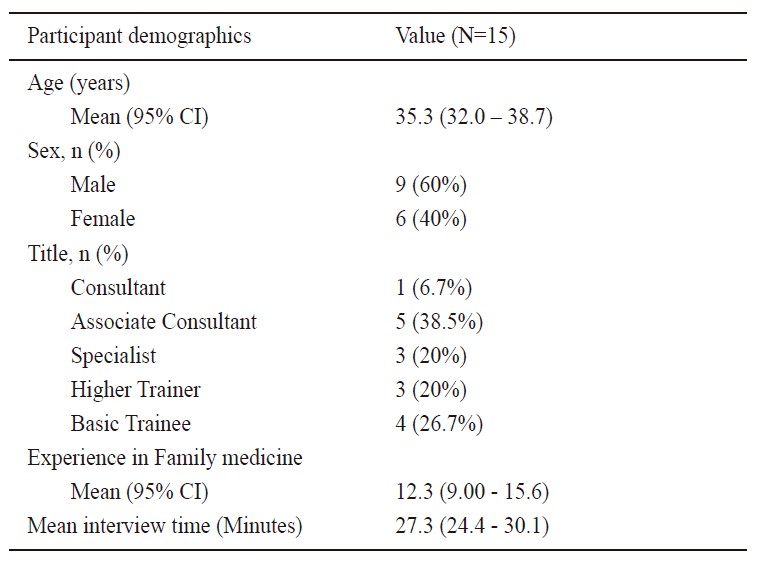
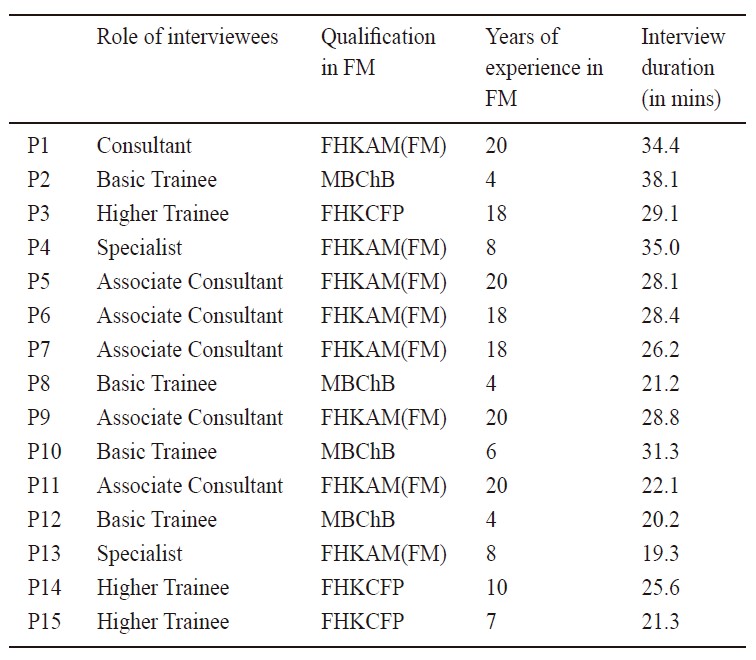
Table 3: Characteristics of each participant
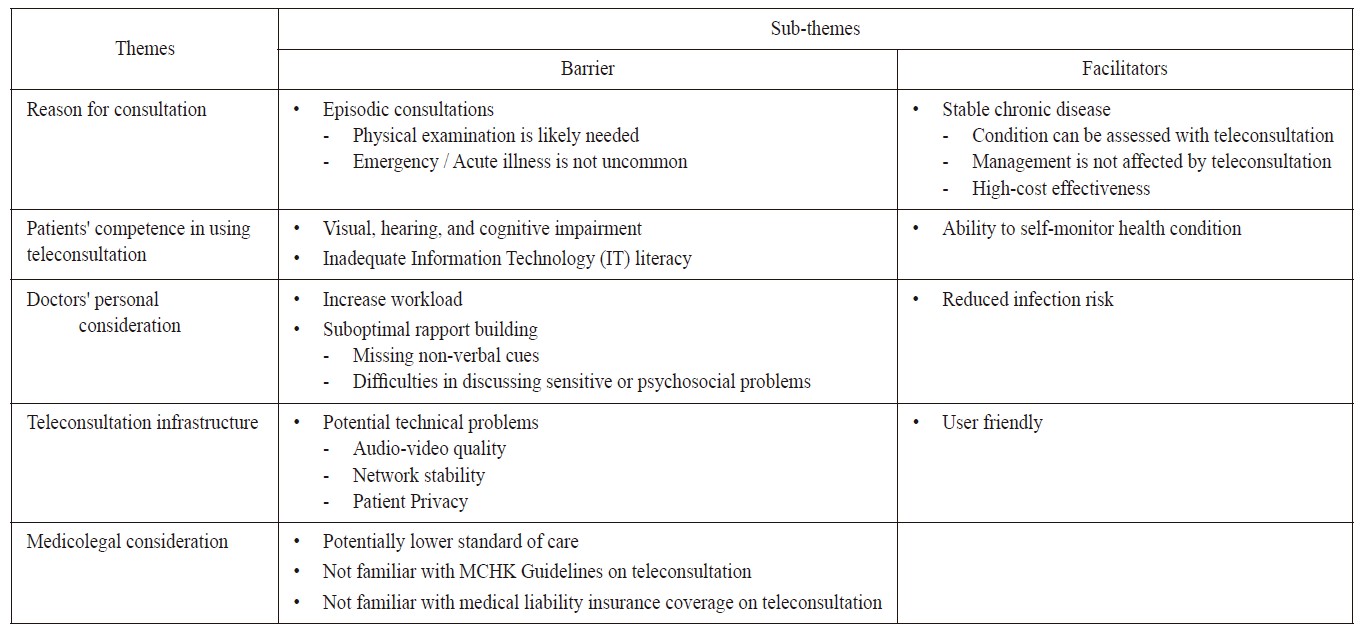
Thematic analysis of the barriers and facilitators identified 5 themes: 1. Reason for consultation, 2. Patients’ competency of using teleconsultation, 3. Doctors’ personal consideration, 4. Teleconsultation Infrastructure, and 5. Medicolegal considerations, as summarised in Table 4.
Reason for consultationThe majority considered episodic consultations as a major roadblock to teleconsultation. Common episodic enquiries including cough, abdominal pain, chest pain, and fever would likely require physical examination (PE), which could not be done during teleconsultation: ‘The reason for consultation is unpredictable. These cases usually require PE. For example, if a patient suddenly complains of cough, we at least need to auscultate the chest. (P6)’ ‘We can call back the patient if PE is needed. But it is meaningless to break one consultation into two. Why don’t we ask them to come in the first place? (P4)’ They elaborated that emergency or acute illness was not uncommon in episodic consultations but immediate investigation and treatment could not be provided via teleconsultation: ‘We cannot do tests like urine multistix, H’stix, ECG, SpO2 or treatment like dressing. (P8)’ ‘From the patients’ perspective, they want immediate medical attention… From the doctors’ perspective, we want immediate PE, investigation, and treatment. (P5)’ In contrast, the majority considered patients with stable chronic diseases as good candidates for teleconsultation. Examples included hypertension, diabetes mellitus, hyper/hypothyroidism, and mood disorders because they could be reliably assessed by teleconsultation: ‘No need for PE in those cases. You can ask about history, drug compliance, blood pressure, etc. through the screen. (P8)’ ‘There are clear disease targets (blood pressure, H’stix, weight) which patients can easily provide through teleconsultation. The assessment for these conditions is usually standardised. (P1)’ In addition, they explained that the routine management for these conditions would not be affected by teleconsultation: ‘Provided that they can do self-monitoring properly, teleconsultation should be equal to real consultation. The way we titrate medications is similar. (P2)’ ‘Immediate onsite investigation or treatment after consultation is usually not needed. (P5)’ Some participants considered practicing teleconsultation on stable chronic diseases as more cost-effective than episodic diseases: ‘Patients with stable chronic diseases are prevalent in our clinic, and they will be under our care for a long time. It would be worthwhile training them to use teleconsultation. (P1)’ Table 4: Summary of Barriers and Facilitators for implementation of teleconsultation
Patients’ competence in using teleconsultationThe majori ty had concerns about patients’ ability to use teleconsultation as many patients in their practice were old and some suffered from different degrees of visual, hearing, and cognitive impairment. ‘Hearing, speaking, or cognitive problems affect their communication ability, especially during teleconsultation. (P3)’ ‘Face-to-face observation picks up non-verbal cues better, and PE plays a more important role in these patients than others. (P4)’ The majority were also concerned with inadequate IT literacy among these elderly patients for teleconsultation. ‘Our elderly patients’ IT proficiency is not good. There could be a lot of hiccups leading to a waste of time. It is difficult to help them from afar. (P11)’ ’No matter how well we prepare for teleconsultation, everything will be pointless if patients face hardware or software problems. (P2)’ Some participants reported greater motivation to do teleconsultation with patients who were able to self-monitor health conditions: ‘If patients can self-monitor figures like blood pressure and H’stix and transmit them to us, it would be more helpful.’ (P2) ‘It empowers the patient in self-monitoring which would improve selfmanagement of chronic illnesses (P1)’.
Doctors’ personal considerationThe majority said teleconsultation would increase workload related to case selection, inefficient consultation, and patient training, which decreased doctors’ motivation to use it. ‘There is a lot of work screening suitable cases for teleconsultation via triage questions, home self-monitoring readings and laboratory results. (P9)’, ‘If patients need to come another time for PE, I won’t have fresh memory about important points that I thought of initially. History needs to be reconfirmed. (P2)’ ‘It takes extra time to train patients to use teleconsultation. (P12)’ Some participants suggested suboptimal rapport building would decrease doctors’ motivation to use teleconsultation: ‘Patients’ traditional idea is to see a doctor face-to-face. Teleconsultation will affect rapport building making it more difficult for doctors and patients to agree on a management plan. (P6)’ ‘It is difficult to sense non-verbal cues and assess and manage psychosocial problems through teleconsultation. (P5)’ ‘Sometimes, patients do not feel comfortable talking about sensitive history in front of cameras. (P9)’ In contrast, half of the participants mentioned reduced infection risk of COVID would increase their intention to use teleconsultation: ’It reduces our contact with patients and clustering of patients in a clinic. (P6)’ ‘Teleconsultation may be suitable for assessing asymptomatic/mild COVID cases. (P8)’
Teleconsultation InfrastructureThe majority pointed out that potential technical problems were major barriers. Their negative experience with audio-visual quality and network stability with currently available videoconferencing platforms adversely affected their confidence in using teleconsultation: ‘The unstable audio-visual quality, stuttering or disconnection etc. will impact the quality of the consultation when patients give important information. (P12)’ Most participants suggested user-friendliness would be essential to encourage the use of teleconsultation: ‘User-friendliness is important. Training to use the tool is important too. (P1)’ In addition, concerns about patient privacy were also raised:’ IT security and hackers make me concerned. Data privacy problems will cause big trouble for the patient and us. (P5)’
Medicolegal considerationsThe majority were reluctant to provide teleconsultation due to potentially lower standard of care which would cause medicolegal liability. It was because of the lack of physical examination, immediate surgery test and treatment for the patient: ‘The standard of care for teleconsultation needs to be the same as real consultation. If some physical signs are missed, there will be medicolegal problems. (P2)’, ‘Lack of PE, surgery test, and immediate treatment are known limitations of teleconsultation. (P9)’ Also, suboptimal rapport with patients was considered a risk factor for medicolegal problems: ‘Suboptimal communication would increase the risk of facing medicolegal issues. (P4)’ The majority reported that they were not confident with teleconsultation because they were unfamiliar with the MCHK Guidelines on teleconsultation. Some said they have no chance to learn ‘The seminars were during working hours. How can we attend? There is not enough promotion about it for us. (P3)’ Others read through the guidelines but wanted further clarification: ‘The guideline is vague. It just said doctors should maintain the standard of care during teleconsultation (P10).’ ‘It is too general. The recommendation is just like that for traditional consultations. (P8)’ The majority had similar comments about insurance problems as they were also unfamiliar with medical liability insurance coverage on teleconsultation:’ It is essential to know if we are covered by medical liability insurance and to have a formal seminar introducing the scheme to us. (P4)’
Discussion
Summary of findingsBarriers to implementing teleconsultation perceived by our Family Physicians include episodic consultations, patients’ inability to use teleconsultation, increased workload (due to case selection, inefficient consultation, and patient training), perceived suboptimal rapport building, potential technical problems, potential lower standard of care, and unfamiliarity with current MCHK guidelines on teleconsultation. Facilitators included follow-up consultations for stable chronic diseases, patients with the ability to self-monitor their health condition, lowering infection risk, and user-friendliness of teleconsultation platform. At the end of the interviews, only 3 out of 15 participants said they were ready to provide teleconsultation. The majority who were not ready explained that the barriers must be addressed first.
Compare with existing literaturesLowering infection risk was a newly identified facilitator in our study, which was reasonable considering the COVID-19 pandemic. Teleconsultation allows practice of social distancing which reduces cross-infection between doctors and patients while maintaining as much clinical service as possible. Other findings were consistent with overseas literature. A study on 6 UK primary care practices36 reported that 38.1% of the teleconsultation bookings eventually reverted to face-to-face consultations mostly due to enquiries about new conditions, or complex questions. Our UK counterparts echoed with workload concerns due to screening teleconsultation requests and reversion to face-to-face consultation after first teleconsultation.23,36 Therefore, careful case selection by a nurse-led triage system will be discussed in “Clinical Implications”. Patients’ competence in using teleconsultation was a common concern in our participants. This concurred with existing literature that difficulty in using technology, especially with elderly patients, was a major barrier to teleconsultation.23 Effective teleconsultation follow-up also necessitated patients to do self-monitoring for disease parameters.21 For patients who are unable to use teleconsultation device or do self-monitoring, a caregiver may be important in overcoming their barriers. Some of our participants raised concerns about suboptimal rapport, which echoed with previous studies on views of clinicians with limited experience in teleconsultation. 21,37 However, Donelan et al. showed that after actual engagement with teleconsultation, 59% patients and 51% doctors considered rapport to be same as face-to-face consultations.38 Doctor-patient communication is important in relationship building21, and poor sound quality or lighting can inhibit communication.37 These can be improved by a wellplaced microphone to improve verbal communication, and diffuse lighting without glare to observe facial expressions and non-verbal cues.39 Regarding teleconsultation infrastructure, our participants identified user-friendliness as a facilitator and potential technical problems as a barrier. Foreign studies reported that staff found it difficult to concentrate on the patients’ needs if they needed to concurrently fix technical issues.20,21 The medicolegal risk was a universal cause of resistance to implementing teleconsultation.31 Participants were hesitant in teleconsultation as they were unfamiliar with the current regulatory guidelines40 and medical liability insurance policy. Staff education should overcome this barrier.
Strengths and limitationsThis study focused specifically on views on implementing teleconsultation by Family Physicians in Hong Kong. Addressing barriers and facilitators perceived by local staff is key to implementing teleconsultation21 as it would increase their intention to use new technology.22 There are limitations with this study. Firstly, being a single cluster study, the results may not be fully generalisable to other HA clusters despite sharing similarities. However, an increase in heterogenicity results in a substantially larger sample size and resources were a significant barrier in this study. Nevertheless, this can serve as a pilot study for other clusters. Secondly, most participants lacked teleconsultation experience when they are interviewed in early 2021 as teleconsultation was generally not available in the public primary care at that time. While this study aimed to understand public Family Physicians thereby motivating them to use teleconsultation, the smooth implementation of teleconsultation would also benefit with experience from other teleconsultation providers. Private Family Physicians who provide care to a great number of patients with acute episodic illnesses with teleconsultation experience can be interviewed in future studies. Their experience may provide useful information for the public sector ’s reference. Thirdly, for data analysis, if resources allow, investigator triangulation should be done to improve credibility which involves two investigators independently performing thematic analysis. Any disagreement should be addressed by a third investigator.
Clinical implicationsTo address the barriers identified in this study, implementation strategies are suggested as follows. A triage system should be established for careful patient selection. In the initial phase, patients with eligible chronic diseases including HT, DM, hyperlipidaemia, hyper/hypothyroidism, and mood disorders under the public primary care can apply for teleconsultation via the current one-stop mobile app (HA Go). They will need to provide self-monitored disease parameters (e.g. BP, Weight, H’stix) via the app and declare any adhoc episodic problems. If they are not familiar with video-calling by mobile phones, they will be advised to invite caregivers to accompany them. The triage staff will review their medical records to exclude unstable cases requiring PE or surgery tests, and cases with known visual, hearing, or cognitive impairment. These measures will help minimise the possibility of calling back for a second consultation inducing unnecessary workload. Triage nurses should be recruited for this new service to avoid overloading existing staff. Training videos on the usage of the teleconsultation platform will be provided via HA Go. Patients will need to test their mobile phone’s video, audio, and network function via the app beforehand. An encrypted videocall session with queuing system will be established via the app. A pilot run of teleconsultation will be conducted to troubleshoot technological difficulties. Traditional consultation quotas will be reserved for timely and necessary conversion back from teleconsultation to maintain the quality of care. Stable chronic cases managed by teleconsultation should come back at least once yearly for onsite assessment (PE, investigations). It will also improve rapport which may increase patient satisfaction and reduce medicolegal risks. Lectures regarding the MCHK teleconsultation guideline should be provided as part of the vocational training by the employers. Relevant insurance agencies e.g. Medical Protection Society should be invited to host case discussions and illustrations to enhance doctors’ competency and confidence to apply it to their practice.
ConclusionThis study explored important facilitators and barriers perceived by our Family Physicians. The implementation process of teleconsultation should address the major issues including careful case selection, taking staff ’s personal consideration into account, refining the teleconsultation IT infrastructure, and providing medicolegal support. The COVID-19 pandemic has disrupted medical care for many patients, but teleconsultation can alleviate this. Hopefully, this study would provide insight into helping Family Physicians, the gatekeeper of patients’ health, embrace ‘the new normal’.
AcknowledgementThe author would like to thank Dr. Leung Kwan Wa, Dr. Leung Shuk Yun, Professor Sit Wing-shan, Dr. Chung Kin Wing, Dr. Choi Yue Kwan, Dr. Lee Sum, Dr. Yau King Sun for their precious advice contributed to this research. Key messages
References
Appendix A – Teleconsultation interview guide
Barriers and facilitators to the implementation of telemedicine-based, real-time, online consultation (teleconsultation) among family physicians working in the public sector. Thank you for participating in this study. I am Dr Yan from Family Medicine of New Territories East Cluster. The interest of this study is to understand the opinion of Family Physicians on implementing teleconsultation in this department. Therefore, you are invited to this interview to share with us your understanding of the barriers and facilitating factors for using teleconsultation in the public sector. I am going to ask you some questions. There are no right or wrong answers. Please do not feel like you must answer in a certain way. Please let me known at any point when you feel uncomfortable responding to a question. First, let us start by understanding more about your background as a family physician.
Position in the department of Family Medicine Qualification obtained related to Family Medicine (e.g. FHKCFP, FRACGP, FHKAM(FM), DFM, etc) Years of experience working as a family physician As teleconsultation service is not yet available in the public sector of family medicine, to facilitate the discussion, and here is a service model of teleconsultation that is commonly used. Let’s assume similar service will be provided if telemedicine is implemented in the public sector. The patients who want to make an episodic appointment of teleconsultation can use pre-existing booking system (e.g. telephone booking system, smartphone application) The patients who have a scheduled follow up can call the clinic to indicate the preference to have teleconsultation. A dedicated doctor will be assigned to have only teleconsultation within a single consultation session. The teleconsultation will be conducted with video conferencing software like Zoom. After the consultation, a logistic team will be responsible to deliver medications, documents to the patients (sick leave certificates, referral letters). If further face to face consultation is needed (e.g. for physical examination), another consultation will be arranged at the clinic. Base on this scenario, I am going to ask some questions. Q1. Can you tell me your experience in using teleconsultation? Possible probes: You can share any experience with us. As a user? As a service provider? Q2. Can you tell me your learning experience about teleconsultation? Possible probes: Seminars, trainings, online research, journals, books, etc. What did you learn about the teleconsultation? If we are going to implement teleconsultation in this department, I would like to know what are the factors that will encourage you to or stop you from using teleconsultation. Let us start with the system users. (Internal Factors) Q3a. What kind of patients do you prefer to use teleconsultation with? Why?
Q3b. What kind of patients do you prefer not to use
teleconsultation with? Why?
Q4a. What will encourage you as a doctor to use teleconsultation? Potential probes: What are the personal considerations that motivate you to use teleconsultation?
Q4b. What wil l discourage you as a doctor f rom us ing
teleconsultation?
Q5a. What are the important features of the teleconsultation platform (the one that you use to communicate with the patient) that will facilitate you to use the system? Q5b. What are the potential technical problems that you foresee with the teleconsultation platform? Q6a. What are the potential medical legal problems with using teleconsultation? How do they affect your choice on whether or not to practice teleconsultation? Q6b. What do you know about the current medical liability insurance coverage with regards teleconsultation? How does that affect your choice with practicing teleconsultation? Q6c. What do you know about the current medical council guideline for teleconsultation? How does that affect your choice on whether or not to practice teleconsultation? Q7. Are you ready to provide teleconsultation? Why? Q8. Is there anything that you feel that we have not covered with this topic that you want to share?
Dr. Chi-yung Yan,
FHKCFP, FRACGP, FHKAM (Family Medicine)
Correspondence to:
Dr. Chi-yung Yan, Yuen Chau Kok General Outpatient Clinic,
|
|