|
September 2025,Volume 47, No.3
|
Original Article
|
The knowledge level towards urinary incontinence among community-dwelling Hong Kong Chinese women – a crosssectional studyMinru Li 李敏如,Huali Wang 王華力,Wai-kit Ko 高煒杰,Siu-kei Kwong 鄺兆基 HK Pract 2025;47:64-71
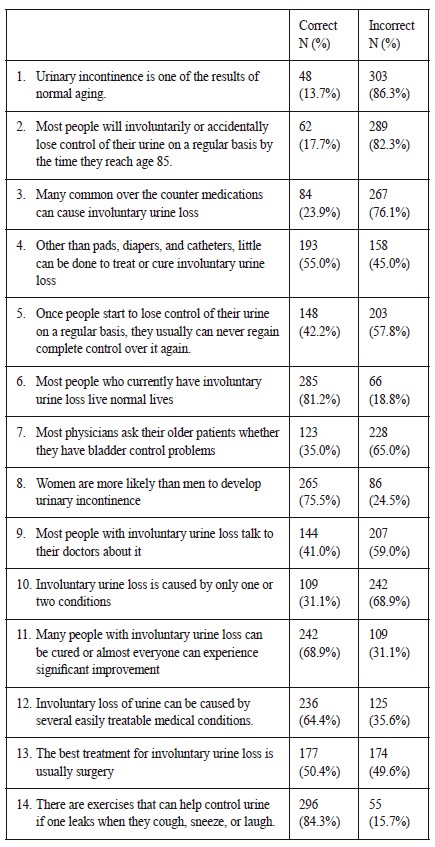
SummaryObjective: To explore levels of urinary incontinence (UI) knowledge among Hong Kong Chinese women and the predictive factors.Design: A cross-sectional study using questionnaires. Subjects: 351 Chinese women with age ≥40 years attended General Out-patient Clinics between 1st May to 30th June 2022. Main outcome measures: The questionnaire consisted of three sections: (1) demographic data, (2) severity of UI and impairment of quality of life (3) knowledge of UI. Methods: Multivariate linear regression was used to calculate the independent affecting factors of demographic status and UI symptoms with knowledge level. Results: 53.2% had symptoms of UI but only 25.0% symptomatic patients sought any doctor consultations. The UI quiz score was 6.82±2.76 (total 14) and the highest incorrect item was “Urinary incontinence is one of the results of normal aging” (incorrect rate 86.3%). Multivariate analysis showed that income (B=1.116, P < 0.001), education level (B = 0.768, P = 0.002) and symptomatic of UI (B = 0.651, P = 0.015) were significant independent impact factor of patient’s knowledge of UI. Conclusions: The knowledge level among Chinese women who attended GOPCs of Hong Kong West Cluster (HKWC) is below average. Misconception of “UI is one of the result of normal aging” is the most prevalent barrier of seeking help. Besides UI symptom, low education level and low income are the predictive factors of having a low UI knowledge level. Community education should be enhanced to improve women’s knowledge and promote them to seek help early. Keywords: Urinary Incontinence, Knowledge, Chinese women
摘要目標:研究香港華裔女性對尿路失禁的認知水平以及其影 響因素。設計:問卷調查的橫斷面研究。 對象:我們把在2022年5月1日至6月30日到普通科門診就診 的351名年齡40歲以上的華裔女性納入作為研究對象。 主要量度目標:問卷主要包括3部分:(1)人口統計學數 據;(2)反映尿路失禁的嚴重程度(UDI-6量表)和生活質量 受損程度(IIQ-7量表);(3)尿路失禁認知水平(尿路失禁量 表)。 方法:使用多因素線性回歸統計人口統計學數據和尿路失 禁症狀對尿路失禁認知水平的獨立影響因素。 結果:研究人群中53.2%有尿路失禁的症狀,但是其中只 有25%的患者諮詢了醫生。尿路失禁認知水平問卷顯示平 均分數為6.82±2.76(總分14分)。其中錯誤率最高的問題 是“尿失禁是正常老化的結果之一”(錯誤率為86.3%)。 多因素分析顯示收入(B = 1.116, P < 0.001),教育水平(B = 0.768, P=0.002)以及有尿路失禁症狀(B = 0.651, P=0.015) 均為尿路失禁認知水平的獨立影響因素。 結論:香港華裔女性對尿路失禁的認知水平並不充分。 “尿失禁是正常老化的結果之一”這個錯誤的認知是影響 病人尋求醫學幫助最主要的阻礙因素。除了患有尿路失禁 外,教育水平和收入低下是影響對尿路失禁認知水平的獨 立因素。因此有必要加強對這部分人群的社區教育,以提 高女性對尿路失禁的認知水平,並促使她們早期尋求醫學 幫助。 關鍵詞:尿路失禁,認知水平,華裔女性 Introduction
Urinary incontinence (UI) is defined as any leakage
or involuntary loss of urine at inappropriate times. UI
is not life threatening, but it can impair the physical,
mental, and social aspects of health.1 The prevalence
rate of UI in women world wide ranges from 25%
to 45%. Our previous study found that besides the severity of UI, the other affecting factor for a patient’s seeking help behaviour was their level of knowledge.6 Henceforth improving population knowledge on this subject may promote a patient’s help seeking rate. Current studies addressing knowledge of UI primarily focused on women presenting to specialists7 or among carer providers.8 Little is known about the knowledge among the general female population and their predictive factors. No quantitative study on the subject of UI knowledge has been performed in our communitydwelling Hong Kong Chinese women. The objective of this study is to determine baseline levels of UI knowledge among adult women presenting to the primary care clinic, and to further assess the predictive factor of knowledge level. Through these findings, we hope to support the planning of educational interventions and improve help seeking rates. MethodsThis is a cross-sectional study using questionnaires. The study was approved by the Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster (HKU/HA HKW IRB) (reference: UW 22-234). Selection criteriaWomen age ≥ 40 years attended the 4 General Outpatient Clinics (GOPC) of Hong Kong West Cluster between 1st May to 30th June 2022 were invited to complete the questionnaire. Exclusion criteria included (1) non-Chinese ethnicity; (2) unable to understand Chinese and (3) refusal to join this study. Information sheets about the study were consecutively distributed to patients who have met the inclusion criteria who attended the aforementioned GOPCs. Patients were interviewed by the principal investigator to complete the questionnaires after verbal consent. QuestionnaireThe questionnaire consisted of three sections: (1) demographic data, (2) knowledge of UI, (3) severity of UI and impairment of quality of life (for symptomatic women).
StatisticsDescriptive statistics were used to summarise demographic characteristics. Continuous variables were expressed as mean ± standard deviation. Categorical variables were expressed as frequency and percentage. Statistical analysis was performed using SPSS 23.0. Chi square test was used to compare the demographic parameter between our group and the female population of Hong Kong. Univariate analysis using one-way ANOVA to assess the relationship of demographic status including age, marriage status, parity, education level, occupation, income level and UI symptoms with knowledge level. Parameter with P < 0.1 were entered into multivariate linear regression to calculate the independent affecting factor of UI knowledge. P value < 0.05 was considered statistically significant. Result:351 patients were included in the study, with the mean age of 61.98 ± 9.99 years old. There was no significant difference in age, income and education level between our group and the 2021 Hong Kong female population census. (Table 1) Table 1: Demographics and past training experience of the respondents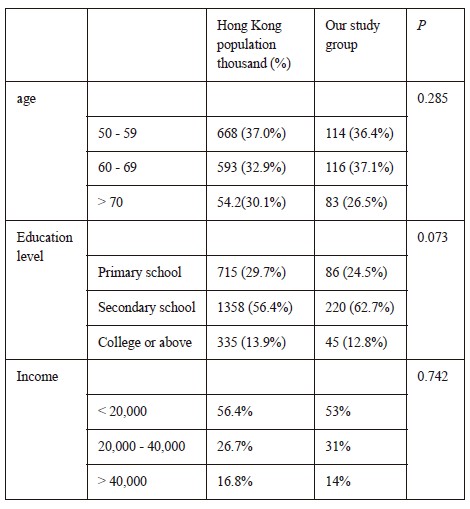
*Data from Women and Men in Hong Kong Key statistics 2022 edition and Thematic report: household income distribution in Hong Kong187 (187/351, 53.2%) had symptoms of UI. Among them, 40.1% (75/187) had mixed UI, 46.0% (86/187) had stress UI, and 13.9% (26/187) had urge UI. UDI-6 mean score was 19.23 ± 12.21. (Table 2) Table 2: Prevalence of urinary symptoms in the study population and the severity of symptoms (UDI-6)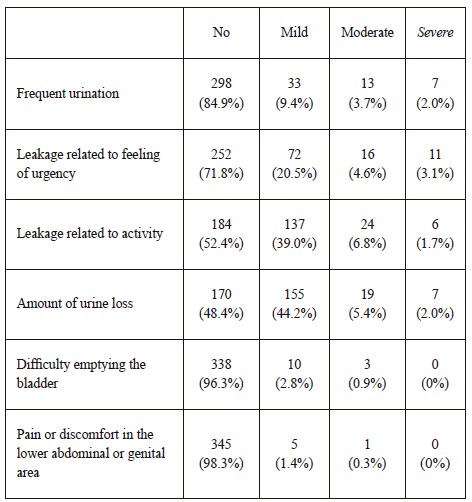
*The mean score of items is multiplied by 33 1/3 to convert to a 0–100 scale.20.9% (39/187) women reported quality of life was affected (IIQ-7 > 0). IIQ-7 mean score was 3.33 ± 9.09 (Table 3). Table 3: Incontinence impact Questionnaire IIQ-7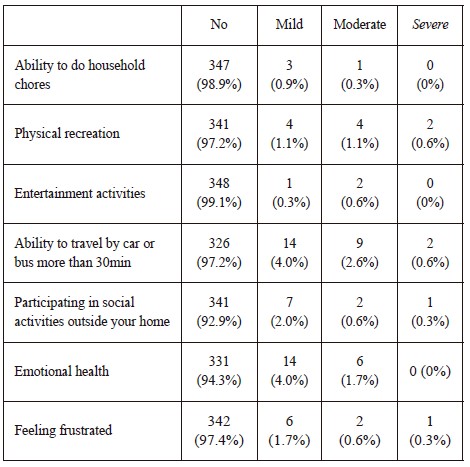
*The mean score of items is multiplied by 33 1/3 to convert to a 0–100 scale.Only 47 of women (47/187, 25.1% ) with symptoms of UI had consulted a doctor, mainly general practitioners (31/47, 66.0%), followed by gynaecologists (13/47, 27.7%) and urologists (3/47, 6.3%).
Table 5: univariate analysis of character association with UI quiz score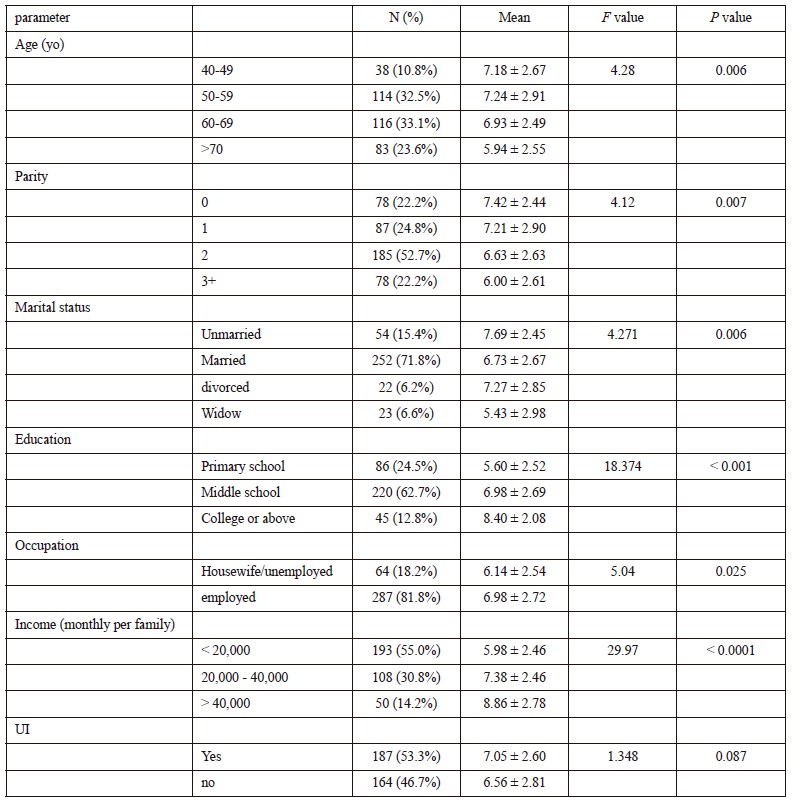
DiscussionParticipants in our study were recruited from 4 GOPCs and were not recruited from the general people of Hong Kong. We compared the demographic data including age, education level and income between the 2021 census of Hong Kong female population and our group, and there was no significant difference found between them. We used UID-6 and IIQ-7 in our study, as these are used worldwide including China and Hong Kong for evaluating urinary symptoms and quality of life with a high sensitivity and specificity.12 Their wide use can help us compare other local studies. There were 53.2% women who suffered from UI and only 25.1% with symptoms of UI seek any doctor consultation regarding this. This was comparable to the literature found on this subject among Chinese women in mainland China1 and was similar to a territory-wide telephone survey done in Hong Kong in 2006.13 In Wong’s study, 16% reported QOL impairment, which was similar to ours (21.9%). Our study suggested that the knowledge level of UI in Hong Kong Chinese women who attended GOPCs in HKWC was below average, with a mean score of UIQ was 6.82 ± 2.76. It was reported that the mean score of UIQ was 9.29 (66.4%) in 18–30-year-old American women14; 6.16 in white and 5.46 in minority women15; and 4.85 in community-dwelling Korean-American women above 30 years of age.16 From our questionnaire, we found that more than 80% of participants thought that urinary leakage was part of normal aging. It was even a little bit higher than the study done in 2006 in Hong Kong16, which reported 75.7%. Studies have found that this misconception was one of the barriers for women seeking help as they do not perceive UI as abnormal. Women also did not have enough knowledge of the cause of UI. The “correct rate” of Q3 (“Many common over the counter medications can cause involuntary urine loss”) and Q10 (“Involuntary urine loss is caused by only one or two conditions”) were only 23.9% and 31.1% respectively. 65% participants mistaken that physicians would proactively ask their older patients whether they had bladder control problems. This misconception also would delay patients in their report of symptoms. For the treatment option, though the questions of this domain had a higher knowledge compared to others. There was still nearly half of the participants who didn’t know UI was treatable or even curable, and thought that surgery was the best treatment. Still 45% patients thought other than pads, diapers, and catheters, little can be done to treat or cure involuntary urine loss. When women encounter urine leakage problem, selfcoping strategies are usually the first action women take to manage UI. In one study, 85% incontinence women were found to rely on the use of pads and adult diapers.17 This strategy, while seems to be a positive action and can keep their quality of life, could worsen UI by preventing them seeking medical help. In the univariable analysis, several demographic factors (age, income, education level, employed, marital status, high parity) were significantly associated with UI knowledge level. While only education level, income and UI symptom retained statistically significance in the multivariate analysis. For Branch et al 9, advanced age seemed to be related to better levels of knowledge about the treatment and consequences of UI. While Chen et al18 found that the age group between 40-49 had a higher knowledge level. We found that population at age 50-59 had the highest score of UIQ and was significantly higher than the age group of 69-69 and > 70. It is similar to Branch’s research. But in multivariate analysis, age was not the significant impact factor, when other demographic factors were taken into account. When we explored the impact of marital status on knowledge level, it is not surprising to find that the lowest level is the widow group. Most of the widow women were elderly. They tended to be less educated and had a lower income. Interestingly, in the univariate study, unmarried participant had the highest knowledge score, while married participants had even lower UI knowledge level than single and divorced women. This could possibly be explained by single persons were more highly educated. In one of the population surveys of Hong Kong, among the women with education level above college, 12.6% women in the 30-40 age group never were married in 1996, while this percentage increased to 16.8% in 2004 (from http://HKCSS.ORG.HK). It is assumed that married women needed to take care of the whole family and pay less attention to their health. Further multivariate analysis showed that marital status was not significant when other demographic factors were taken into account. Key messages
Another interesting result was that nulliparous women had better knowledge than multiparous respondents in the univariate analysis, though this was not statistically significant with the multivariate analysis after balancing other demographic factors. One would expect women to gain knowledge on pelvic floor disorders from previous pregnancies. Maybe early childbearing could be associated with lower education levels and employment. Childcare commitments may also reduce these women’s attention to their own health. Hence, we can give more education led by nurses or physiotherapists on UI through prenatal class. It is not surprising to find that higher education, high income and employed participant will have a higher UI knowledge level. They may have a better access to resources such as the internet, health magazines, articles and interact with their colleagues, all of which could result in an increase in their knowledge on this topic.19 Our multivariate analysis showed that education and income had a significant impact on UI knowledge level. These findings are consistent with several studies.20,21 Therefore, when we face the patient with a low income or education level, we should provide more education and anticipatory care about UI when their attend for a consultation. This might empower them to take responsibility for their condition and treatments. Symptom of UI is another significant impact factor of UI knowledge. Perera’s study22 also found that symptomatic patients had higher knowledge of UI. As for the symptomatic patient, they may pay more attention to information on UI from media or / and friends. Some of them had already sought help from specialist. Hence this all could result in having a higher level of knowledge compared to the asymptomatic patients. ConclusionThe knowledge level among Chinese women who attended GOPCs of HKWC is below average. More than half of the participants were unaware that UI is a disease with the possibility of prevention and treatment. Community education on UI, recognition of early symptoms and creating awareness of available management options may help to encourage women to seek help early. While imparting knowledge can be time-consuming, simple strategies to communicate that UI is not a “natural part of childbirth and aging” can alter perception and knowledge. This is especially when we face those with a low income and a low education level. Community-based educational tools through health talks, pamphlets and public services advertising may help women to be familiarised with UI. References
Minru Li,
LMCHK, FHKCFP, FRACGP, FHKAM (Family Medicine)
Huali Wang,
LMCHK, FHKCFP, FRACGP, FHKAM (Family Medicine)
Wai-kit Ko,
MBBS (HKU), FHKCFP, FRACGP, FHKAM (Family Medicine)
Siu-kei Kwong,
MBBS (HKU), FHKCFP, FRACGP, FHKAM (Family Medicine)
Correspondence to: Dr Minru Li, Department of Family Medicine & Primary Health care,
North Wing, 6/F, Tsan Yuk Hospital, 30 Hospital Road,
|
|