
|
September 2025,Volume 47, No.3
|
Original Article
|
Confidence of family physicians in performing office procedures – a cross-sectional survey from public primary care clinics in Hong KongHenry HH Wong 黃衍熹,Lap-kin Chiang 蔣立建,Susanna LL Hung 孔樂霖,Ka-ming Ho 何家銘,Yim-chu Li 李艷珠, Catherine XR Chen 陳曉瑞 HK Pract 2025;47:72-79
SummaryObjective: To evaluate the self-reported confidence in performing office procedures among family physicians (FP) and to explore its association with FP’s demographics and training experience.Design: Cross-sectional survey conducted in public primary care setting. Subjects: All full-time FPs working in the Department of Family Medicine and General Out-patient Clinics of Kowloon Central Cluster of the Hospital Authority of Hong Kong from 1/6/2021 to 31/12/2021. Main outcome measures: The proportion of FPs reporting confident in performing 10 office procedures and its association with FPs’ demographics or training experience. Results: Totally 89 FPs completed the survey, with an overall response rate of 82.4%. 68 (76.4%) of them graduated locally in Hong Kong, 40 (44.9%) are male, and 40 (44.9%) had practiced for more than 10 years. 38 (42.7%) had completed Family Medicine (FM) basic vocational training, and more than half (50, 56.2%) had previous office procedure training. The mean (SD) of the confidence scores in the 10 office procedures was 2.99 (0.97) out of 5. 61 (68.5%) FPs reported confidence in performing pap smears, while less than half (ranged from 27.0% to 47.2%) reported confidence in performing the other 9 procedures respectively. 12 (13.8%) doctors reported not being confident in performing any of the 10 procedures, while only 4 (4.6%) doctors had confidence in performing all listed procedures. Less than half of the respondents were confident in performing four or more procedures. Completion of FM basic vocational training, surgical rotation and attachment to office procedure training were associated with a higher confidence score. Conclusions: FPs have limited confidence in performing common office procedures in the public primary care setting. Completion of FM basic vocational training, surgical rotation and attachment to office procedure training were associated with better procedural confidence. Keywords: Family physician; Office procedure; Primary care
摘要目的:研究本地家庭醫生施行小型手術的自信程度,以及 探討此自信程度與家庭醫生的背景特徵和訓練經驗之間的 關係。設計:在公立基層醫療進行的橫切面調查研究。 對象:香港醫院管理局九龍中聯網家庭醫學及基層醫療部 的所有全職家庭醫生。 主要量度目標:家庭醫生有自信施行十項小型手術的比 例,和施行小型手術自信程度與醫生的背景特徵和訓練經 驗的關係 。 結果:89位家庭醫生完成問卷,回應率為82.4%。68位 (76.4%)受訪家庭醫生在本地畢業,40位(44.9%)為男性, 40位(44.9%)行醫超過十年,38位(42.7%)完成家庭醫學 專科基礎培訓,過半數(50位,56.2%)曾參與小型手術訓 練。十項小型手術的平均自信分數為2.99(滿分5分,標準 差0.97)。61位家庭醫生(68.5%)表示對施行子宮頸抹片有 信心,而少於一半醫生(範圍27.0%至47.2%)表示有信心 施行其餘九項的小手術項目。12位(13.8%)受訪家庭醫生 表示沒有自信施行所有十項小型手術,4位(4.8%)則表示 對施行十項均有自信。少於一半受訪者表示對施行四項或 更多小型手術有自信。完成家庭醫學專科基礎培訓、外科 輪轉訓練及參與小型手術訓練與更高的自信分數有顯著關 聯。 結論:在公立基層醫療工作的家庭醫生施行常見小型手術 的自信有限。完成家庭醫學專科基礎培訓、外科輪轉訓練 及參與小型手術訓練與提升家庭醫生進行小型手術的自信 有顯著關聯。 關鍵詞:家庭醫生,小型手術,基層醫療 IntroductionFamily Medicine (FM) is a broad-spectrum specialty that encounters a wide variety of diseases including conditions requiring office procedures. In fact, office procedures have been an integral part of primary care worldwide.1-6 The scope of office procedures vary widely from country to country and is likely defined by the medical tradition and the primary care boundary of that country. It ranges from simple procedures such as suturing, cryotherapy, joint injection, ultrasound, to more advanced ones such as excision of skin lesions, reduction of fractures, even to major operations done under general anaesthesia.6 Provision of office procedures has been shown to be favourably received by patients, reduce referrals to hospital care7-8,10 and reduce overall medical cost.9 Nevertheless, a prospective randomised trial has found that the quality of minor surgeries done in the primary care setting is not as high as that carried out in hospitals, especially for malignant lesions.10 It signifies the importance of procedural skill training for primary care doctors to ensure patient safety. However, difficulties exist when it comes to providing procedural skill training.11,12 First, there is a lack of procedural knowledge and skills in graduating medical students and family medicine residents entering training.13-16 Second, while core procedural skills in family medicine training are well defined in countries such as US, Canada and Australia1-3, there is a lack of specific training standards in procedural skills for family medicine residencies in Hong Kong. Third, constraints in time, manpower and resources can limit such training in the public health care setting.19 Lastly, the benefit of procedural skills training may be lost over time, unless there is an ongoing chance to practice and master those learned skills.20 While several studies commonly identified a lack of confidence in performing office procedures among FPs worldwide16-18, there is currently no data exploring such confidence among FPs locally. To fill this knowledge gap, this study aims to evaluate the selfreported confidence in performing office procedures among FPs working in the public primary care setting and to explore its association with FPs’ demographics and training experience. MethodStudy DesignCross-sectional questionnaire survey conducted from 6/2021 to 12/2021. An invitation email with a link to the survey questionnaire was sent to all selected FPs. FPs completed online questionnaire via Google forms anonymously. SubjectsAll FPs working in the Hospital Authority (HA) Kowloon Central Cluster (KCC) Department of Family Medicine and General Out-patient Clinics (GOPCs) were invited to join this study. Part time doctors were excluded as they may not have acquired their procedural skills from the cluster and would not be involve in providing office procedures with their clinical duties. Sample size calculationThe confidence in performing office procedures of local FPs is unknown. A pilot study among ten FPs estimated 30% FPs are confident in office procedures in general. Using an online sample size calculator, assuming 30% of FPs competent in performing office procedures, with alpha value 0.05, estimated effect size 1 and absolute precision 0.1, the minimal sample size was 81. To allow room for exclusion and incomplete data (approximately 20%), 101 FPs were required as the sample size for testing. In total there are 130 FPs working in the Department, excluding 22 part-time doctors, all remaining 108 doctors were invited to join this study. Survey instrumentAs there was no validated local questionnaire available, the author developed a questionnaire with reference to local and international training requirements for family physicians, expert opinions and literature reviews.13-16 It consisted of two parts. The first part gathered basic information on demographics and past training experience related to office procedures of the respondents. The second part contained a list of office procedures specifically for FPs. The author and a group of family medicine specialists involved in training activities reviewed all the priority skills listed in the basic training logbook by the Hong Kong College of FPs (HKCFP). Adopting the definition of an office procedure according to the Royal Australian College of General Practitioners3, 25 procedures were identified. After core group review, the list of procedure was further simplified and refined through a consensus process according to practical considerations and was finalised to ten procedures (Appendix 1). For each procedure, FPs were asked on how many times they have performed them in the past, how confident they are in performing them, whether they think it is important to family medicine, and whether they are interested in further training. The level of self-reported confidence was rated using a 5-point Likert scale (1 = no confidence; 2 = minimal confidence; 3 = can do it, if supervised; 4 = can perform it independently; 5 = can teach the procedure to others). It has been shown that self-confidence scale is psychometrically valid to represent doctors’ selfconfidence during surgical training.21 Appendix 1. Flow chart of office procedures selection process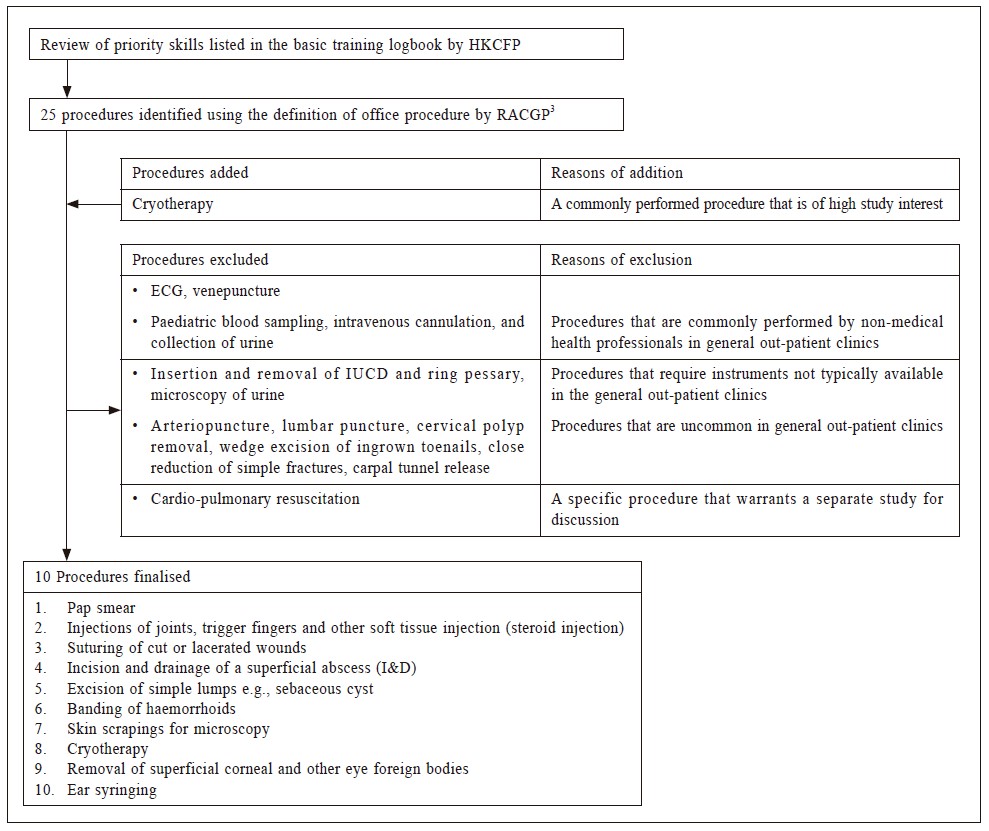
Questionnaire Validity and ReliabilityA core group consisted of experienced FM trainers, FM specialists and family physicians had been invited to comment and review on the questionnaire for relevance and content validity. The questionnaire was pilot-tested in a group of 5 FPs for face validity. Internal reliability analysis was performed on the responses on the number of times performed and self-reported confidence in the 10 office procedures. The internal consistency of the responses was assessed with the Cronbach’s alpha value, which showed the survey had an acceptable level of reliability (alpha value 0.880 [number of times performed] and 0.908 [confidence scale]). Outcome assessmentThe primary outcome of the study was to identify the proportion of FPs reporting confident (>/= 4) in performing each of the 10 selected office procedures, and to identify whether there was any association between self-reported procedural confidence and the FPs’ demographics or past training experience. The secondary outcome was to assess the opinion of FPs on the perceived importance in family medicine and willingness to receive further training in each of the procedures. Statistical analysisAnalysis was performed using IBM SPSS Statistics (version 26). Descriptive statistics was used to report demographics and past training experiences of FPs. For each procedure, the numbers and percentages of FPs who have performed, the reported confidence in performing, the perception of the importance in family medicine, and the willingness to receive training in doing it were listed. A confidence score of more or equal to 4 was considered confident. Student’s t-test and ANOVA test were used for analysing continuous variables and Chi-square test for categorical data. All variables with p-value < 0.2 in the univariate analyses were entered into a multivariate logistic regression to look for the associated factors of better confidence level in performing the office procedures. P-values of less than 0.05 were considered statistically significant. Research ethicsThe study was approved by the Hospital Authority Research Ethics Committee (Reference: KC/KE-20- 0370/ER-1). Potential conflicts of interestThe authors have declared that there are no potential conflicts of interest. ResultsA total of 89 FPs (response rate 82.4%) completed the questionnaire. Table 1 summarises the characteristics of the respondents. 40 of the FPs (44.9%) were male, 68 (76.4%) graduated locally, 42 (47.2%) had either another degree or medical diploma, 38 (42.7%) had completed basic vocational training in FM, and 69 (77.5%), 61 (68.5%) and 56 (62.9%) had completed hospital rotations in Surgery, O&G and Orthopaedics respectively. 50 (56.2%) had attachments to office procedure training that consisted of dedicated clinic sessions performing lump excision, steroid injection, cryotherapy and ear syringing. This is also locally known as minor operations (MOT). Table 1: Demographics and past training experience of the respondents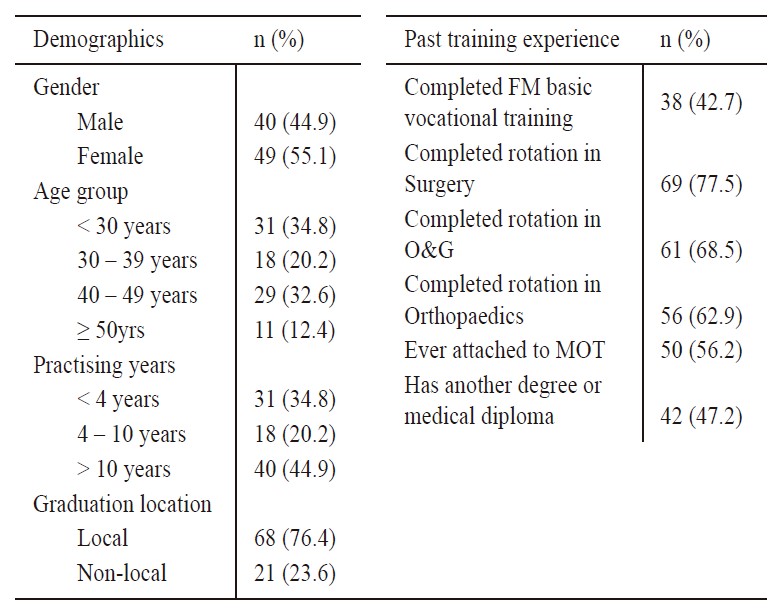
MOT: minor operationThe number of times performed, confident in performing, perceived importance in and training interest in each of the ten procedures are shown in Table 2. Two procedures, i.e. pap smear and ear syringing, were performed more than five times by more than half of the respondents. On the other hand, skin scraping was the least performed procedure, with 64 (71.9%) respondents reported never doing it before. Pap smear was the procedure most respondents were confident in doing (n = 61, 68.5%). The other nine procedures had less than half of the respondents reporting confidence in performing, with skin scrapings being the least (n = 19, 21.3%). All procedures were regarded important by more than 80% of respondents. Steroid injection had the most respondents interested in further training in (n = 74, 84.1%). The mean (SD) of the confidence score in 10 office procedures was 2.99 (0.97). Using the median confidence score (3.2) as a cut-off, respondents were divided into two groups, below median as non-confident group and above median as the confident group. The confidence score according to FP’ demographic data and training experience was studied and summarised in Table 3. Completion of FM basic vocational training, hospital rotation in Surgery, O&G and Orthopaedics and attachment to MOT were significantly associated with above-median confidence score while gender, age group, practicing year, graduation location, and possession of another degree or medical diploma were not. Logistic regression for association factors with p value less than 0.2 showed completion of FM basic vocational training, surgical rotation and attachment to MOT were independently associated with being above the median confidence score (Table 4). Table 2: No. of times previously performed, confidence in performing, perceived importance in, and training interest in 10 procedures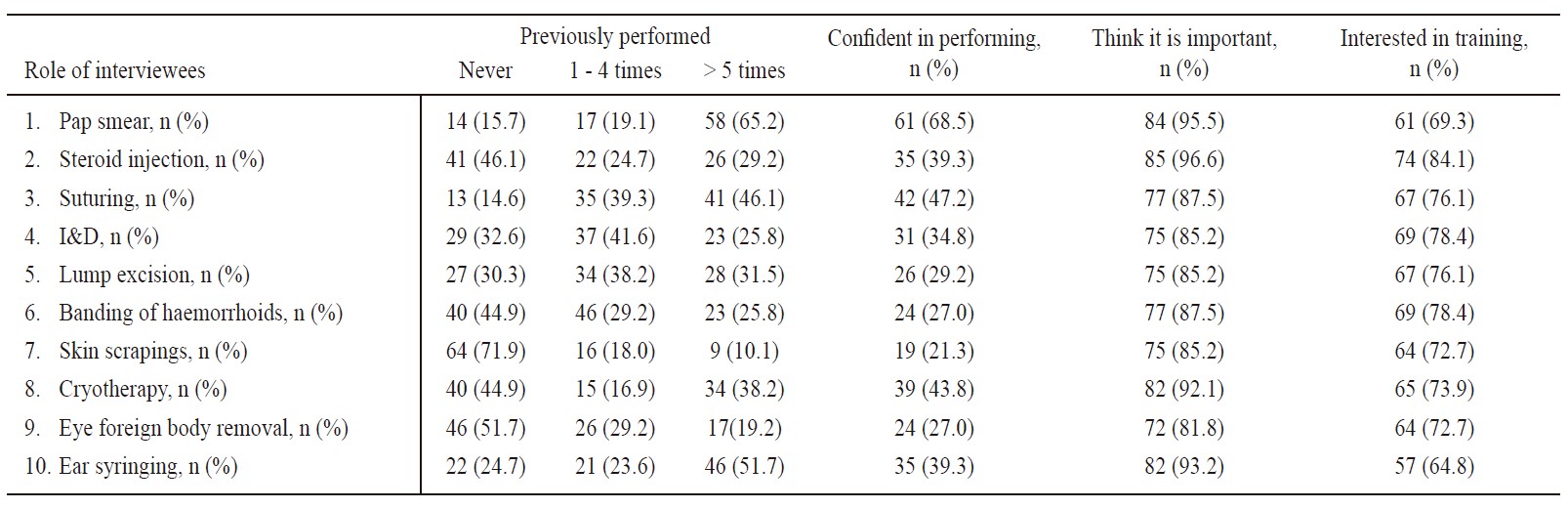
I&D: Incision and drainage of a superficial abscessTable 3: Mean confidence score with respect to demographics and past training experience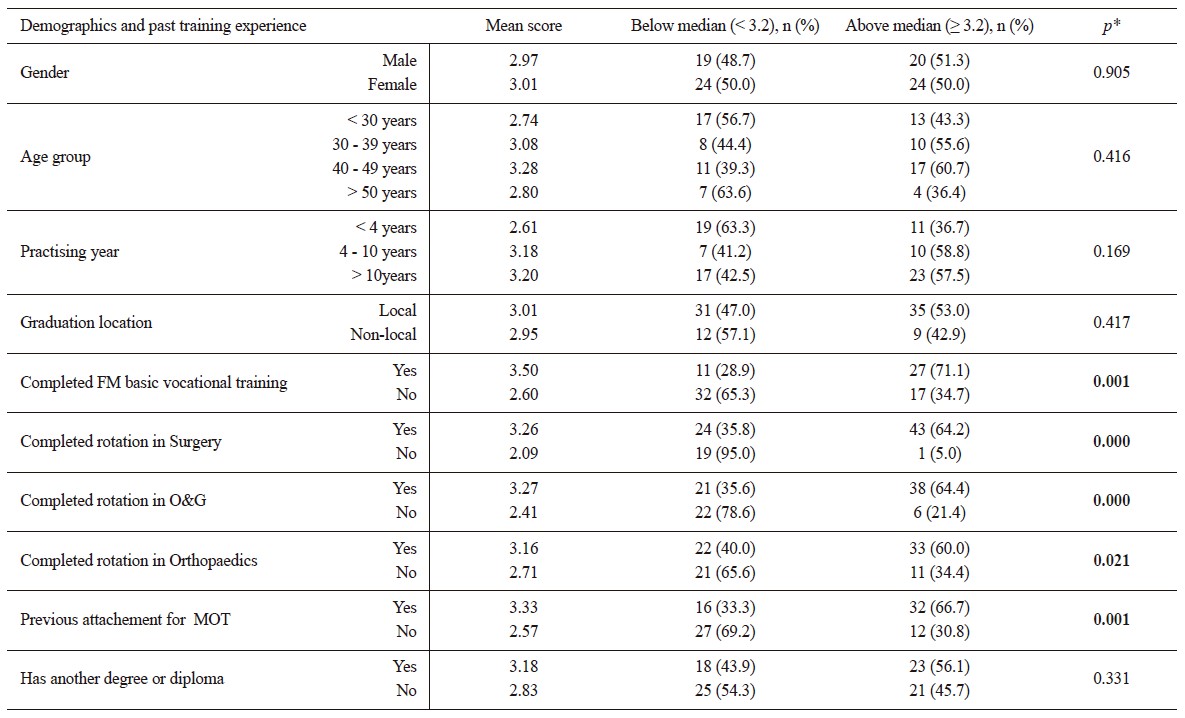
MOT: minor operationTable 4: Logistic regression analysis for associated factors for FPs’ confidence in performing office procedures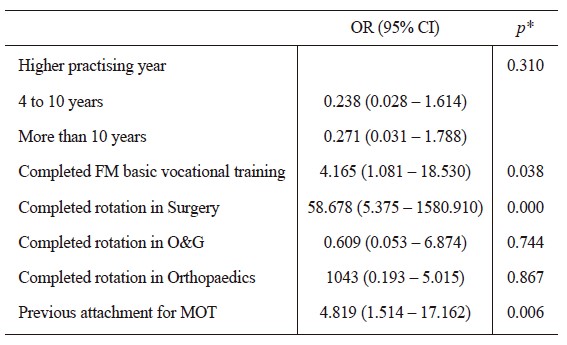
Figure 5 shows the distribution of respondents being confident in performing each of procedures. There were 87 respondents in total, more than half of the respondents (45 out of 87, 51.3%) expressed confidence (confidence score ≥ 4) in three or less procedures. Twelve FPs (13.8%) reported being confident in none of the procedures, and 4 of them (4.6%) reported being confident in all of the 10 office procedures. Figure 5: No. of procedures the respondents were confident in performing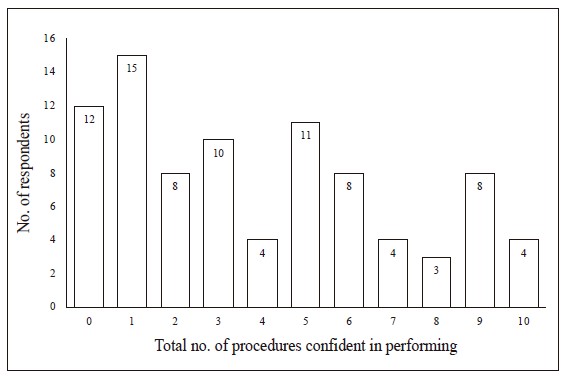
DiscussionFM doctors are expected to achieve competency in performing common off ice procedures upon completion of vocational training of HKCFP. All of the ten procedures selected from the training logbook were perceived to be important to the practice of FM by most of our respondents (> 80%). This showed that the view of FPs in our study was in line with the expectation of the HKCFP. However, more than half of FPs in this study could only perform three or less office procedures independently. Alarmingly, 12 FPs (13.8%) have no confidence in doing any of the procedures. This reflects that local FPs generally have a significant deficiency in the skills needed for performing important office procedures. This finding is consistent with studies on FPs elsewhere.16-18 The mean confidence score in performing office procedures of local FPs (i.e. 2.99) was comparable to two studies, with one ranged from 2.34 to 3.7316, and another one at 3.2.18 although the scope of studied office procedures may be widely different. The reasons contributing to this lack of confidence in performing office procedures are multi-factorial. First of all, there is limited hands-on exposure in performing office procedures in the public primary care clinics. For example, I&D of a simple abscess can be performed by the family physician in the clinic. However, due to time constraints and inadequate of facilities, the patients were usually referred to AED for further management. Of the ten studied procedures, only two were performed more than five times by more than half of the respondents. Secondly, consultation time constraint and manpower limitations in the public primary care setting is another important barrier to the provision of adequate office procedures during our daily practice.19 The average consultation time allocated for each case in GOPCs is about 6 to 7 minutes, which had posed a great challenge to the FP if he or she has to finish the consultation as well as the procedure within such a short time. Thirdly, some doctors included in this study were relatively junior and have not received adequate training. For example, 57.3% of the respondents have not completed basic FM vocational training. Additional procedural training for FPs may be necessary to enhance their exposure to common office procedures. Our study identified completion of basic FM vocational training, hospital rotation in Surgery, and attachment in MOT were the only three factors associated with a higher confidence score. While it is not surprising that basic FM vocational training and surgical rotation have important roles in procedural skills training, our study suggested the potential training value of MOT sessions in order to enhance the procedural skills of our FPs. Unlike surgical rotation which is only accessible through vocational training programmes, MOT sessions could be available to all FPs regardless of training status. Considering around half of our respondents have never had any attachment for office procedure training, setting up more MOT sessions in various community clinics and the provision of regular procedural training attachments for our doctors could open up more opportunities for them to learn and practice common office procedures. It could also satisfy the high training interest of doctors in our survey for steroid injections. A follow-up study comparing the pre and post-attachment confidence level may be needed to further confirm the training role of MOT sessions. Key messages
Strength and limitationsThis is the first study in Hong Kong to explore the confidence of FPs in performing office procedures and has provided important background information for HKCFP as well as HA to further improve its training and service development. In addition, the study’s good response rate, i.e. 84.2%, has significantly geared a strength for this survey. However, there are several limitations of this study. First, as all FPs were recruited from one local cluster in the public primary care setting, the findings of this study may not be generalised to all FPs or private doctors in Hong Kong. Second, as the reliability and validity of the survey questionnaire had not been fully evaluated, accuracy of these findings need to be interpreted with caution. Lastly, the self-reported number of times performed and confidence levels may have a recall bias. Future studies with more FPs from both public and private sectors, and a wider range of studied office procedures are necessary to better reflect the procedural confidence of FPs in Hong Kong. ConclusionDespite office procedures being an important aspect of FM practice, our study found that FPs working in the public primary care setting had limited experience and confidence in performing these common procedures. To fill in this service gap and to meet the increasing service demand, additional training programmes targeting at improving FPs’ procedure skills in HA is recommended. Set-up of minor operation sessions in primary care clinics and enhanced training via regular clinic attachment will help enhance FPs’ confidence in performing common office procedures in primary care. References
Henry HH Wong,
FHKAM (Family Medicine)
Lap-kin Chiang,
MBChB, FHKCFP, FRACGP, FHKAM (Family Medicine)
Susanna LL Hung,
LMCHK, FHKCFP, FRACGP, FHKAM (Family Medicine)
Ka-ming Ho,
MBBS, FHKCFP, FRACGP, FHKAM (Family Medicine)
Yim-chu Li,
MBBS, FHKCFP, FRACGP, FHKAM (Family Medicine)
Catherine XR Chen,
MRCP (UK), PhD (HKU), FRACGP, FHKAM (Family Medicine)
Correspondence to: Dr. Lap-kin Chiang, 1/Floor, Tsui Tsin Tong Outpatient Building,
Kwong Wah Hospital, 25 Waterloo Road, Mongkok,
|
|