|
June 2007, Volume 29, No. 6
|
Original Articles
|
The Chinese Quality of Life instrument: reliability and validity of the Hong Kong Chinese version (ChQOL-HK)Sau-Li Zhao 趙利, Kwok-fai Leung 梁國輝, Kelvin Chan 陳金泉 HK Pract 2007;29:220-232 Summary
Objective: (1) To undergo translation and linguistic validation
of the Mandarin Chinese version of the ChQOL into Hong Kong Chinese version; (2)
to assess the psychometric properties of the Hong Kong Chinese version of the ChQOL.
Keywords: Chinese Quality of Life Instrument, Cross-cultural, Reliability, Validity 摘要
目的: (1)將漢語版本的「中華生存質量量表」(ChQOL)翻譯為廣州話(稱為香港版本),並確定其語言學上的正確性;(2)評定該香港版本在心理測量學上的特性。
主要詞彙: 中華生存質量量表,跨文化,可靠性,正確性。 Introduction The Chinese Quality of Life instrument (ChQOL) is a self-reported health status generic measurement specifically developed as an outcome measure for Chinese medicine. Its development was based on the concept of health in Chinese medicine. This is one of the very few instruments which were developed on a clear and explicit theory of health in the context of the Chinese culture. The ChQOL consists of 50 items in 3 domains (physical function, spirit and emotion) and 13 facets (complexion, sleep, stamina, appetite and digestion, climate adjustment, consciousness, thinking, spirit of the eyes, verbal expression, joy, anger, depressed mood, fear and anxiety). The domain and facet structure of the ChQOL is shown in Figure 1. The items are the manifestation of the equilibrium of Ying and Yang of correspondence facets and domains. The ChQOL uses a 5-point Likert scale to rate the intensity, frequency, or evaluation of the selected attributes of health status. All facet and domain scores are transformed to reflect on a 0 to 100 scale, a higher score indicating a better health status. It was first developed and validated in Mainland China. Previous studies revealed that the structure of the ChQOL was valid and the psychometric properties were good.1,2 It could provide additional information of health on top of some other generic health related quality of life instruments, i.e. the WHOQOL-100 and the SF-36.1,2 As a result of the geographical, political and cultural separation of Mainland China and Hong Kong for over 100 years, the Chinese characters may be different between Mainland China and Hong Kong. Up to 2001, ninety-five percent of the population in Hong Kong is Chinese, their written language is Chinese, and the daily spoken language is Cantonese. Only 34% of the population can speak Mandarin.3 Translation into Hong Kong Chinese and testing for cross-cultural validity are required before the ChQOL can be applied to the people in Hong Kong. The aims of this study were (1) to undergo translation and linguistic validation of the Mandarin Chinese version of the ChQOL into Hong Kong Chinese version; (2) to assess the psychometric properties of the Hong Kong Chinese version of the ChQOL. If these tests are confirmed, the ChQOL-HK would potential apply to Chinese people living in Hong Kong as well as to those who have migrated from Hong Kong to other countries. We hope that our work will stimulate a wider use of ChQOL as a health and outcome measure in the care of nearly one quarter of the world's population who is Chinese. Methods We followed standard translation procedure and pilot testing of the questionnaire.4,5 The first stage was translation of the Mandarin version into the Hong Kong Chinese language and evaluation to ensure conceptual equivalence and respondent acceptance, to produce a form that could be used in data collection. The second stage was formal psychometric tests of the ChQOL-HK to ensure that this was applicable to the people concerned. Firstly, 4 bilingual individuals, who were familiar with both Hong Kong Chinese and Mandarin, were invited to perform forward translation of the questions from written Mandarin in the original ChQOL to written Hong Kong Chinese independently. These translators had a clear and detailed understanding of the instrument and the population who would use the instrument, thus the instrument could be translated more appropriately, the language level used in the translated document could match closely with the target group.5 A native speaker of the target language is a better translator than someone who learned it as a second language because a native speaker is aware of nuances in expressing the target language.6,7 The translated version was worded in such a way that it was as close to the written language that we used in daily life as possible, so that people of low educational level could comprehend the questions covered. After the 4 translations were produced and collected, an item-drafting bilingual panel, consisting of experts of interview and assessment, clinicians and behavioural researchers, particularly anthropologists, reviewed the 4 translated materials. They looked for inconsistencies between the source language version and the translated document, then they discussed and resolved issues related to the maintenance of the integrity of the source instrument in terms of conceptual, semantic and technical equivalence. They reviewed the items and provided their inputs in writing, shared their comments with one another, considered the points made by each other and reconciled any differences of opinion. The draft ChQOL-HK was then developed. Before the administration of the survey, it is necessary to evaluate the forms and procedures to see if people can actually perform the tasks required. Items that can be understood and answered in a laboratory setting do not imply that they will work in practice. Therefore, a pilot testing was performed to further ensure the quality of translation. Four subjects of different age, sex, and educational levels were invited to complete the draft questionnaire. These subjects were likely to use the instrument in the target culture and would be potential subjects in the proposed studies. The interviewers then invited respondents for comments and opinions on the style, form and other aspects of the questionnaire. For cognitive evaluation, the interviewers went through the questionnaire item by item with the subjects to see if they understood the questions. They were asked to describe in their own words what the question asked for and how they arrived at their answers. If there was any misunderstanding or problems with the questions, the subjects were asked to suggest how the questions should be asked. The bilingual group then considered the comments of these subjects and incorporated them into the translated document. It was at this stage that the linguistic analyses outlined above could be usefully done. This group would also ensure that the document was grammatically correct in the target language. The final version of the questionnaire for use in field test was produced and compared with the original version of the ChQOL. A prospective study was carried out among 122 subjects with 53 healthy subjects and 69 patients having chronic illness in Hong Kong. Healthy subjects were recruited from the community and patient subjects were recruited from several medical clinics. All the subjects involved were adults from 18 to 65 years old, and were able to read and understand the instrument. The instrument was not suitable for people who might not understand the instrument, such as those who had cognitive impairment due to brain damage, dementia, and mental retardation, etc. Data were collected using the ChQOL-HK and the Hong Kong Chinese version of the WHOQOL-BREF (WHOQOL-BREF (HK)). Additional demographic information such as gender, age, education level, self-reported health state, and self-reported disease state was also included. All instruments were self-administered in the same order in booklet form. The retest study was conducted on all the subjects within two days. WHOQOL-BREF (HK) is a generic instrument measuring four separate dimensions of quality of life. It was used as a comparison instrument. Good reliability and validity has been demonstrated in Hong Kong.8 Answers to the two questionnaires were scored according to the instructions and computer programmes provided. The test-retest reliability was evaluated by intra-class correlation coefficients (ICC) for each facets and domains. Cronbach's a coefficients were used in order to evaluate the internal consistency of each facet and domain. The validity of the two questionnaires was examined by Pearson's correlation coefficients between similar dimensions of the ChQOL-HK and the WHOQOL-BREF (HK) questionnaires. The t-test was used to examine the differences in facets and domains between patients and healthy subjects. A p-value of <0.05 was considered as statistically significant. Results A total of 122 subjects were recruited including 69 patients and 53 healthy subjects. About half of the subjects were male (45.9%). The mean age was 38.97 and ranged from 18 to 65. There was no statistically significant difference between the patient and healthy subject groups in gender, mean age, education level and living area. The self-reported disease status of the patient group was significantly worse than the healthy subject group. The self-reported health status of healthy subject group was significantly better than that of patient group (Table 1). In the scale properties of the ChQOL-HK, the mean facet scores ranged from 42 in the complexion facet to 68 in fear facet; Mean domain scores ranged from 57 in the physical form domain to 61 in the emotion domain. The ceiling and floor effects were very small which indicated ChQOL-HK could be applied to subjects with a wide range of health status (Table 2). Test-retest reliability study was conducted on 122 subjects within two days. The ICC(1,1) values ranged from 0.77 to 0.88 in the facet scores, and from 0.89 to 0.90 in the domain scores. The ICC(1,1) value for the overall ChQOL score was 0.92. All facets and domains with ICC value above 0.75 were regarded to have good test-retest reliability. The results on internal consistencies of the facets and domains were all good. Cronhach's alpha values of the facets ranged from 0.70 in the climate adjustment facet to 0.90 in the thinking facet. Cronhach's alpha values for the three domains ranged from 0.73 in the physical form domain to 0.83 in the spirit domain. It was found that the ICC value was better and Cronbach's a value was similar as compared to the source tool - the ChQOL (Table 3). Convergent and concurrent validities were studied by correlating the domain scores of the ChQOL-HK with the self-reported health status (5-point scale ranging from very good to very poor) of the four domains of the WHOQOL-BREF (HK). The three domains scores of the ChQOL-HK had fair to moderate correlation with the four domain scores of the WHOQOL-BREF (HK). All the correlations were statistically significant. The physical form domain had higher correlations with the physical health domain (r=0.709) and had lower correlation with the psychological (r=0.497), social relationship (r=0.306) and environment (r=0.390) of the WHOQOL-BREF (HK). The spirit domain had higher correlation with the psychological (r=0.533) and had lower correlation with the physical health (r=0.461), social relationship (r=0.309) and environment (r=0.434) of the WHOQOL- BREF (HK). The emotion domain had higher correlations with the psychological (r=0.619) and physical health domain (r=0.568), and had lower correlation with the social relationship (r=0.444) and environment (r=0.291) of the WHOQOL-BREF (HK) (Table 4). The correlation between three domain scores and the self-reported health status were fair to moderate. The correlation coefficients were 0.587 in the physical form domain, 0.301 in the spirit domain and 0.453 in the emotion domain. All correlations were statistically significant (Table 4). Facet to domain correlation ranged from 0.644 to 0.778 in the physical form domain, 0.781 to 0.859 in the spirit domain, and 0.702 to 0.891 in the emotion domain. The facet to overall score correlation ranged from 0.432 to 0.713. There was relatively high correlation for the domain and its corresponding facets (Table 5). There were moderate correlations among the domain scores. Correlation between the physical form and the spirit domain, and the emotion domain were 0.425 and 0.608 respectively. Correlation between the spirit domain and the emotion domain was 0.361. There were high correlations between the overall score and the three domain scores. The correlation coefficient ranged from 0.794 to 0.805 (Table 5). Confirmatory factor analysis was done on the questions of each of the facets and the domains to test the fitness of the order item-facet/facet-domain structure. The overall of fitness of the item-facet structure was more than 0.9 except complexion facet (0.847). The overall fitness of the facet-domain structure was more than 0.9. This indicated the construct validity of the ChQOL-HK was satisfactory (Table 6). Compared with patients and healthy subjects so called "known groups", there were statistically significant differences in 6 out of 13 facet scores, physical form domain score and emotion domain score. The results were not satisfactory comparing with the source tool - the ChQOL (Table 7). Discussion The rigorous and comprehensive process of adaptation ensured that most of the problems associated with translation were satisfactorily resolved.9 Revision by an expert group and focus groups identified items which would not be culturally applicable in Hong Kong. The integrity of the ChQOL's conceptual and psychometric properties was preserved. At present, there were no ceiling and floor effects noted. Internal consistency of the facets and domains were all higher than 0.70. The intra-class correlation between test and retest were above 0.75 for all facets and domains. More importantly, the results of internal consistency and test-retest reliability were similar to those obtained with the Mandarin version of the ChQOL. The findings of the study also suggest that the ChQOL-HK has acceptable validity. Pearson correlations among the ChQOL-HK domains and WHOQOL-BREF(HK) domains were moderate to high in the hypothesized direction. It is satisfactory to discriminate the different known groups for facet and domain scores. Limitations of the present study included the fact that the subjects were drawn from convenient samples. The small sample size might also influence the results, especially the statistical significance of the differences found. Nonetheless, for the purpose of testing the effectiveness of the translation and determining the psychometric comparability of the Hong Kong version, samples such as those included in the present study are typically used and have proven to be useful here. In general, the test-retest interval should be long enough so that memory of the first test has minimal influence on the second test; but the interval should not be too long that the trait being measured undergoes real change between the two tests. Most experts recommended two days to two weeks.10 So the interval used in this survey, i.e. two days, was determined from experience in other related studies.11 Further research will include determining the clinical applicability of the ChQOL-HK by assessing the instrument's sensitivity to changes in health status before and after clinical interventions. Conclusion The study demonstrated that the ChQOL-HK achieved acceptable conceptual equivalence with the original ChQOL in measurement, as well as similar reliability and validity, thereby providing preliminary evidence of the overall equivalence of the ChQOL-HK with the original instrument. The good psychometric properties suggest that it may be used in Hong Kong to assess the health and health care needs. Nevertheless, some aspects need further confirmation in clinical trials in Hong Kong, including the instrument's ability to discriminate between specific illness groups, as well as the responsiveness of the instrument. Acknowledgements This study was supported by a faculty research grant provided by the Hong Kong Baptist University. The authors of this study are grateful to Ms Wai-wah Wong for her professional help in translation review, Mr Eric Ziea, Ms Hung-ngan Wong for translation, as well as Ms Ngar-ting Lui for assistance with data collection. Key messages
Li Zhao, PhD
Instructor, School of Chinese Medicine, The Chinese University of Hong Kong, Hong Kong. Kwok-Fai Leung, Manager Department of Occupational Therapy, Queen Elizabeth Hospital. Kelvin Chan, PhD, DSc, CBiol, FIBiol Head of Pharmacy and Chair Professor of Pharmacy and Pharmacology, School of Applied Sciences, University of Wolverhampton, United Kingdom. Correspondence to : Dr Li Zhao, 1/F, Sino Building, Chung Chi College, School of Chinese Medicine, The Chinese University of Chinese Medicine, Shatin, N.T., Hong Kong.
References
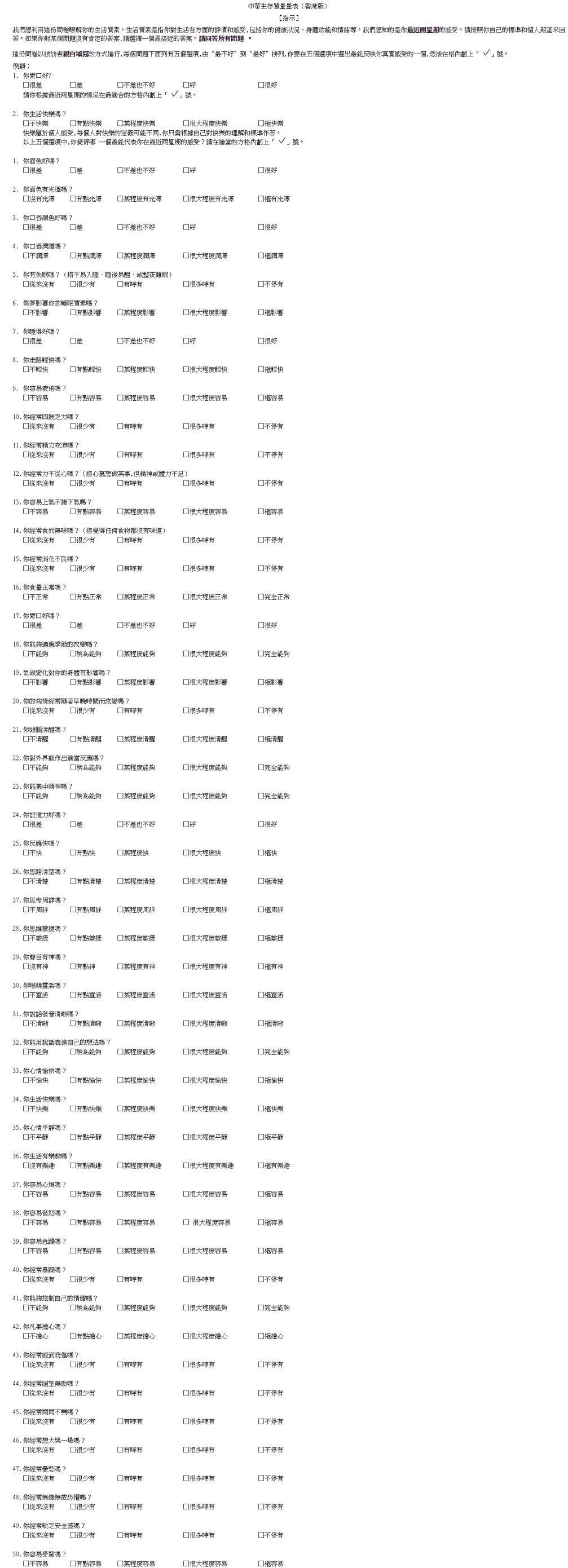
Appendix
|
|