June 2008, Vol 30, No. 2 |
Case Report
|
Two Chinese gentlemen with lung cancer presented with chest painKen K M Ho 何家銘, M S Ng 吳明勝, Alvin C Y Chan 陳鍾煜 HK Pract 2008;30:100-104 Summary Lung cancer is now the most common neoplasm in the world. It could present with very non-specific symptoms. Working in the general out-patient clinics, the consultation time of family physicians is very limited. Hence, the principles of patient management are very important for us to ensure that our patients are getting the most effective and safest management. We report two local Chinese patients who presented with chest pain as the initial complaint of lung cancer. We also discuss the different presentations of lung cancer and illustrate the importance of the principles of patient management. 摘要 肺癌是世界上最常見的腫瘤,症狀表現可以缺乏特異性。因普通科門診家庭醫生診症時間十分有限,為確保病人得到最有效而安全的治療,堅持診治的基本原則非常重要。 本文報告2例最初主述為胸痛的本地華裔肺癌病例,討論肺癌的不同表現,闡述了病人治理基本原則的重要性。 Introduction Lung cancer is now the most common neoplasm in the world according to the National Cancer Institute.1,2 It is also the most frequent cause of death by cancer. As a family physician, making a diagnosis of lung cancer can be very difficult. It is because lung cancer could present with very non-specific symptoms and it is not uncommon for lung cancer to be diagnosed incidentally by chest X-ray. The stage of disease at diagnosis would be the most important factor for survival. The prognosis of the disease depends on how early the tumour is discovered and managed. Delay or inappropriate referral does reduce the survival chances of the patient with lung cancer. Hence, a family physician should not only be responsible for making the diagnosis of lung cancer but should also make sure that the patient was referred appropriately. As we know, consultation time is limited in a busy clinic like our general out-patient clinic. On average, we spend five to eight minutes with each patient. However most of the patients will bring more than one complaint to us. How could we ensure patient safety within the time constraint? This case presentation would highlight four important principles of patient management:
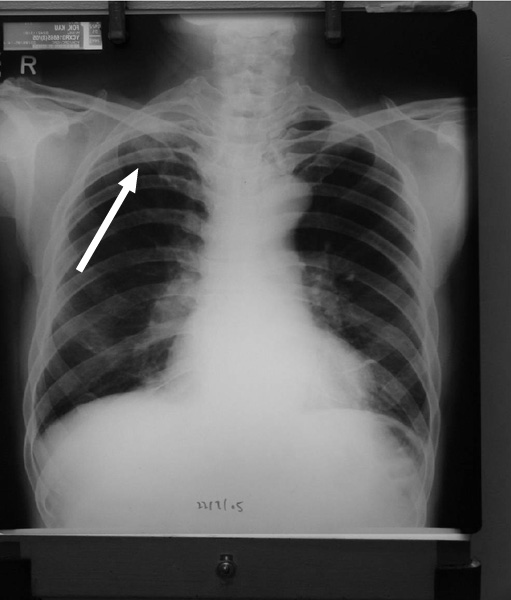
We are going to illustrate these important principles through case reporting of two local Chinese patients who presented with chest pain as the initial complaint of lung cancer. Case 1 A 50-year-old driver with good past health presented in July 2007 with chest pain and productive cough for 10 days. The chest pain was retrosternal and constricting in nature with no radiation. He did not complain of any shortness of breath, palpitation or syncope. There were no aggravating or relieving factors. There was no history of trauma. He did not complain of any acid reflux symptoms. The cough was productive without haemoptysis. He complained of subjective weight loss but his appetite was normal. He was a chronic smoker and chronic drinker at that time. He expressed worry regarding lung and liver cancers as his friend just passed away recently because of cancer. Clinical examination revealed a medium-built gentleman in good general health. He did not have any palpable cervical lymph nodes or finger clubbing. Examination of cardiovascular, respiratory, abdominal, and neurological systems did not show any abnormal findings. He was diagnosed to have musculoskeletal pain and hence an oral analgesic and cough mixture was given. Advice against smoking and drinking was also given. He returned two weeks after the inital consultation indicating that the symptoms were not improved with medication. Chest X-ray and ECG were ordered because of the history of prolonged chest pain and productive cough. He was called back for follow up one week later. The chest X-ray showed an ill-defined opacity in the left upper zone obscuring the contour of the aortic knuckle, which could be due to a perihilar mass or an aortic lesion. He was advised to attend for further investigations such as CT scan (Figure 1). The ECG was normal with no detectable abnormality. He was then referred to the medical department, with an initial appointment given for June 2008. He was called back again for an advancement of appointment because of the serious nature of his illness. In the meantime, he had sought another opinion from a private doctor and had a private CT of his thorax performed on 29th August 2007. This CT revealed a large necrotic mass with encroachment of his left upper lobe bronchus. PET scan showed that the mass was hypermetabolic in nature. He was therefore referred to the Cardiothoracic unit of a public hospital for further management by the private doctor. He was admitted to the Cardiothoracic unit for a mediastinoscopy. The mediastinoscopy revealed right paratracheal and precarinal lymph nodes. He is still currently under the care of this unit. Figure 1 Mr Fok, a 68-year-old gentleman presented to us with a one month history of right shoulder and chest pain. His pain was not related to movement and was described as "tightening" in nature. There was no nocturnal pain. There were no aggravating or relieving factors. There was no history of injury. The other joints were asymptomatic. Concerning his past health, he was a known dementia sufferer and was taken care of by his local psychogeriatric team. He also had an acoustic neuroma which was treated by radiotherapy. Despite all these conditions, he was still able to maintain an independent activity of daily living. He was a retired construction site worker living with his wife. He was a chronic smoker and social drinker. Physical examination of his right shoulder was normal. There was a mild tenderness over the right side of the chest wall around the 2nd and 3rd intercostal space and right scapular region. Chest and cardiovascular examinations were unremarkable. Musculoskeletal pain was diagnosed and managed. He was advised to return in 1 week if the pain persisted. He came back to our clinic ten days later. There was persistent stretching pain which could only be partially relieved with analgesics. Still, there were no aggravating factors. However, he started to have nocturnal pain. Physical examination was again unremarkable. The atypical features of prolonged, non-mechanical nocturnal pain made the diagnosis of simple musculoskeletal pain unlikely. A CXR was ordered to rule out any lung pathology (Figure 2). Figure 2 The CXR showed that there was a newly found ill-defined opacity over the right apex Discussion Lung cancer is the most common fatal malignant disease worldwide and in Hong Kong for both sexes.1-3 There is a global increase of lung cancer by about 2% per year, accounting for approximately 1.2 million new cases annually.2 The principal risk factor is smoking. The lifetime risk of the disease in smokers is approximately 15%.1 Lung cancer could present in different ways.3 It could be an incidental radiological abnormality. Besides this, the presenting symptoms could be due to a primary lesion, intrathoracic spread or distant metastasis. The patient could have constitutional symptoms or systemic non-metastatic syndrome. The key diagnostic feature of primary lung cancer is persistent cough. A study found that the most common initial symptoms were cough and systemic symptoms, followed by dyspnoea, chest pain and bloody sputum.4 Chest pain and cough were more common in the early years. The cough could be caused by the primary bronchial mucosa ulceration or lymphatic spread along both lungs, a phenomenon called lymphangitis carcinomatosis. On the other hand, the chest pain could be due to pleural invasion, pleural effusion or spreading of tumour to chest walls and ribs. If there is pain in the shoulder and arm, there may be brachial plexus (C8 T1 T2) and inferior cervical sympathetic ganglion spread. Chest pain could also be a symptom of cardiac metastasis. There is a case report of lung cancer simulating an acute myocardial infarction because of its spread to pericardium and myocardium.5 It is usually silent. Prognosis is poor. Apart from chest pain and cough, the patient could present with dyspnoea and palpitation. Physical findings may include a pericardial rub or pulsus paradoxus. ECG findings may show regional ST-segment elevation or T-wave inversion. Serum CPK levels could be within normal range. Elevated troponin levels may be observed with pericarditis. Thoracic MRI is indicated to rule out neoplastic infiltration of the myocardium. For our patients, they both presented with chest pain as the first presentation of lung cancer. As the patients presented with chest pain, ECG was performed to rule out acute coronary syndrome. The persistent cough in the first patient could be due to bronchial mucosa involvement or lymphangitis carcinomatosis. The chest pain in both patients could be due to invasion of the parietal pleura with referred pain or brachial plexus with referred pain. The initial presentations of both patients were quite undifferentiated with the initial diagnoses of musculoskeletal pain for both patients. Both cases illustrated the importance of continuity of care. Time was used as a diagnostic tool in both cases. Both patients were advised to attend follow up if symptoms persisted. Further investigations were ordered when the symptoms persisted or when alarming symptoms evolved such as nocturnal pain in the second patient. A study showed that a short time to referral, an incidental diagnosis, a diagnosis not prompted by dyspnoea, by chest pain, by systemic or metastatic symptoms were all associated with a better clinical outcome.4 Hence, the appropriateness of referral could make a significant effect on patient's survival after the diagnosis. Referral implies a transfer of responsibility for some aspect of the patient's care.6 For a family physician, the transfer of responsibility is never a total one, for he or she always retains an overall responsibility for the patient's welfare. A family physician should have a role to ensure that the patient receives the most appropriate referral including an appropriate professional review within an appropriate time interval. A successful referral depends on good communication amongst the primary care physician, consultant and patient; and good communication is a reflection of the degree of integration among the primary, secondary, and tertiary sectors of the health services. For the first patient, the medical appointment was about ten months after a suspected diagnosis of lung cancer with an abnormal chest X-ray. The survival of the patient may have been compromised if he had not been called back for further attention before the scheduled medical appointment. A study which analyzed the principal reasons for a delay in the diagnosis of lung cancer revealed the following list as the most likely causes of delay: 1) Reporting of inflammation or benign tumour by CT scan resulting in a follow-up gap, sequential findings of a lesion with slow growth rate or no significant change; 2) suspicion of lung neoplasm, the malignancy of which was falsely ruled out by a transbronchial biopsy; 3) suspicion of lung cancer followed by the refusal of the patients to undergo a thoracoscopy or further investigations; and 4) dropping out of the follow-up programme.2 The evolutive characteristics of the lung neoplasm and factors associated with the doctor, health system, or patient, can be held responsible for any delayed diagnosis and inefficacy in increasing the survival of these patients. The over-loaded public secondary care in Hong Kong could result in a significant delay in the further management of the patient by a respiratory specialist. It would be our responsibility as family physicians to ensure that our referred patients obtain the most appropriate referrals. Conclusion Our patients have illustrated chest pain as the presentation of lung cancer. Chest pain is an undifferentiated symptom with many differential diagnoses. As a family physician, the continuity of care does let us use time as a diagnostic tool for delineating symptoms. The presence of red flags or atypical presentations would prompt us to take further actions. Moverover, our care should never end with the referral. For the best interest of the patient, we do have the responsibility to make sure that those high-risk patients have been appropriately referred and assessed within a reasonable time frame. Key messages
Ken K M Ho, MBBS(HK) M S Ng, MBBS(HK), Dip Med(CUHK), FHKCFP, FRACGP Alvin C Y Chan, MBChB(CUHK), FRACGP, FHKCGP, FHKAM(Family Medicine) Correspondence to: Dr Ken K M Ho, c/o General Practice Clinic, Yan Chai Hospital, Tsuen Wan, NT, Hong Kong SAR. References
|
|