
|
March 2024,Volume 46, No.1
|
Case Report
|
Vitamin B12 deficiency presented with loss of taste in primary careKa-ming Ho 何家銘, Ka-yan Or 柯嘉茵, Catherine XR Chen 陳曉瑞, Yim-chu Li 李艷珠 HK Pract 2024;46:14-18 SummaryVitamin B12 deficiency is a common condition encountered in primary care. One important cause of vitamin B12 deficiency is pernicious anaemia (PA). The clinical presentation of vitamin B12 deficiency varies, ranging from asymptomatic or very subtle to significant life threatening conditions. Here we report a case of a gentleman who presented with loss of taste in primary care. Blood tests reviewed pancytopenia with severe vitamin B12 deficiency due to PA.
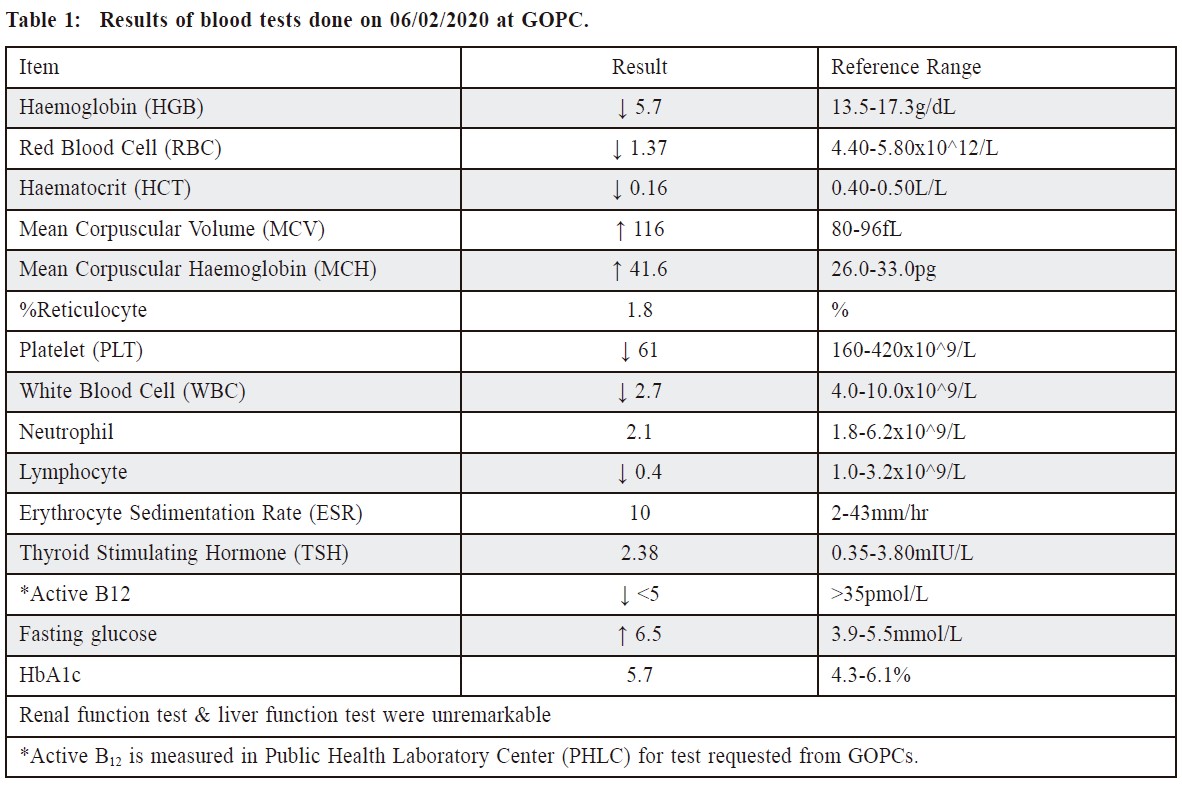
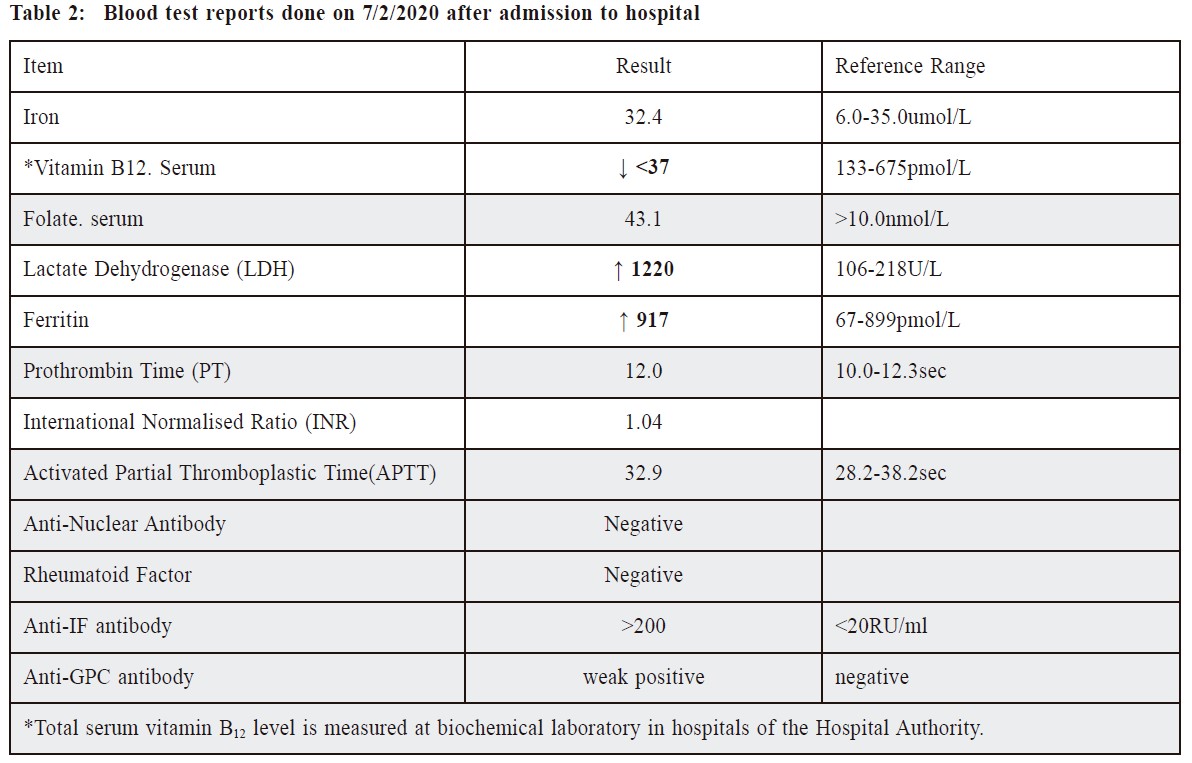
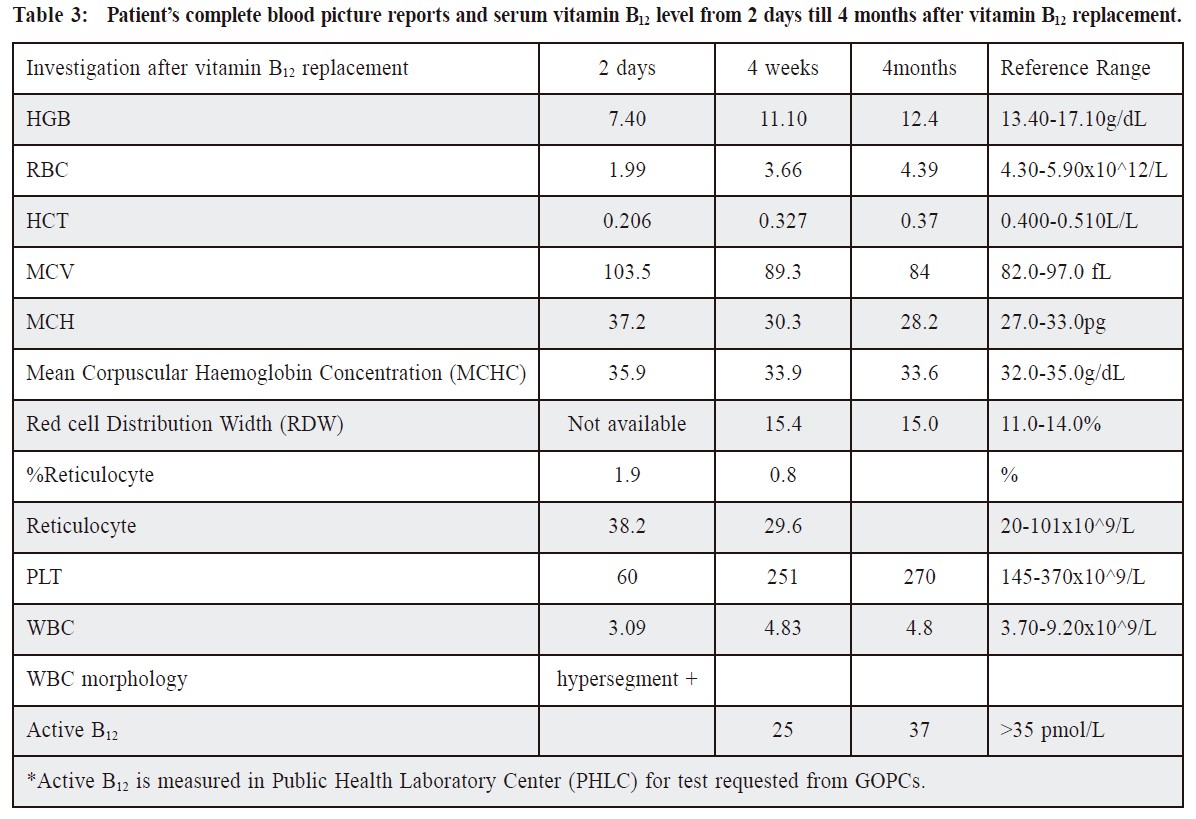
摘要維他命B12缺乏症是基層醫療常遇到的情況。而惡性貧 血(Pernicious Anaemia) 是維他命B12缺乏症的其中一個主要 原因。維他命B12缺乏症的臨床表徵是多樣化的,可以是沒 有任何症狀至出現嚴重致命的併發症。這個案例報告會分 享一個男士因失去味覺到門診求診。及後經血液檢查發現 罹患因惡性貧血引致維他命B12缺乏症併發全血細胞減少症 (Pancytopenia)。 IntroductionVitamin B12 deficiency is a common condition encountered in primary care. Its prevalence gradually increases with age. For example, the prevalence of vitamin B12 deficiency is approximately 6% in persons younger than 60 years, and nearly 20% in those older than 60 years in the USA or UK.1 Locally, the prevalence of vitamin B12 deficiency ranged from 6.6% to 34.9%.2 It can be caused by decreased food intake or malabsorption, autoimmune conditions especially PA, medications e.g. metformin or acid suppressing medications and genetic disorders. The clinical presentation of vitamin B12 deficiency can be quite vague and nonspecific. Patient might be asymptomatic, but could progress to life-threatening conditions e.g. acute myelopathy or pancytopenia if not timely diagnosed and managed. PA is an autoimmune disorder with auto-antibodies against intrinsic factor (IF), gastric parietal cells (GPC), or both. Its prevalence is about 50-4000 cases per 100,000 persons,3 affecting 0.1% in general population and 2% in adults > 60 years old,3 both sexes equally.4 PA is an important cause of severe vitamin B12 deficiency, accounting for 20-30% of documented cases.5 A local study found PA was the second commonest cause of vitamin B12 deficiency after metformin-related vitamin B12 deficiency in the elderly.6 The CaseMr. MTS is a 68-year-old taxi driver, social drinker and non-smoker. He has known history of hypertension, hyperlipidaemia and impaired fasting glucose and has been regularly followed up (FU) in a General Outpatient Clinic (GOPC) of the Hospital Authority since 01/2009. He has been on lifestyle modifications for his chronic illness with satisfactory blood pressure (BP) control all along. He attended our clinic on 05/02/2020 for an episodic visit and complained of loss of taste for one month. The onset of the taste change was insidious associated with xerostomia. There was no pain or ulcer over the tongue, and he did not have cough, sore throat or fever prior to the condition. Mr. MTS is a non-vegetarian. His appetite has been normal, and there was no dyspepsia, abdominal pain or tarry stool. There was no polyuria, polydipsia or weight loss. Systemic review showed that he had no slurring of speech, anosmia, decrease hearing, limb numbness or weakness or gait disturbance. There was no hand tremor, palpitation, diarrhoea, skin rash or genital ulcer. There was no family history of autoimmune disease and he did not take any over-the-counter medications or herbs. Physical examination showed that Mr. MTS was afebrile, his vital signs were stable. The general condition was satisfactory, there was apparent pallor but no jaundice. The tongue mucosa appeared normal without leukoplakia, erythroplakia, ulcer or fissuring. Throat exam was normal and there was no palpable cervical lymph node. Abdominal and neurological exams were both normal. In view of the one-month history of loss of taste and pallor, baseline blood tests were arranged with results shown as follows (Table 1). The reports on 06/02/2020 showed that Mr. MTS had suffered from severe pancytopenia with a very low haemoglobin level of 5.7g/dl. His vitamin B12 level was also remarkably low. Otherwise, the renal, liver, thyroid function tests and sugar level were all normal. Therefore, Mr. MTS was called back urgently and referred for hospital admission immediately. After admission, further blood tests were performed and summarised in (Table 2). The reports showed Mr. MTS had suffered from severe Vitamin B12 deficiency, an elevated anti-IF antibody level and weakly positive anti-GPC antibody. Otherwise, the iron and folate level, clotting profile and other autoimmune markers were all normal. The diagnosis of Vitamin B12 deficiency due to PA was made, blood transfusion and parental vitamin B12 were given immediately. Bone marrow aspiration (BMA) examination was done urgently which showed features compatible with megaloblastic anaemia. Elective oesophago-gastro-duodenoscopy (OGD) was booked to rule out the presence of gastric malignancy. Mr. MTS was advised to have continued FU in GOPCs with lifelong vitamin B12 replacement. After 4 months of monthly intramuscular injection (IMI) of vitamin B12, his blood test in 6/2020 showed that the haemoglobin level and serum vitamin B12 level had both returned to normal (Table 3).
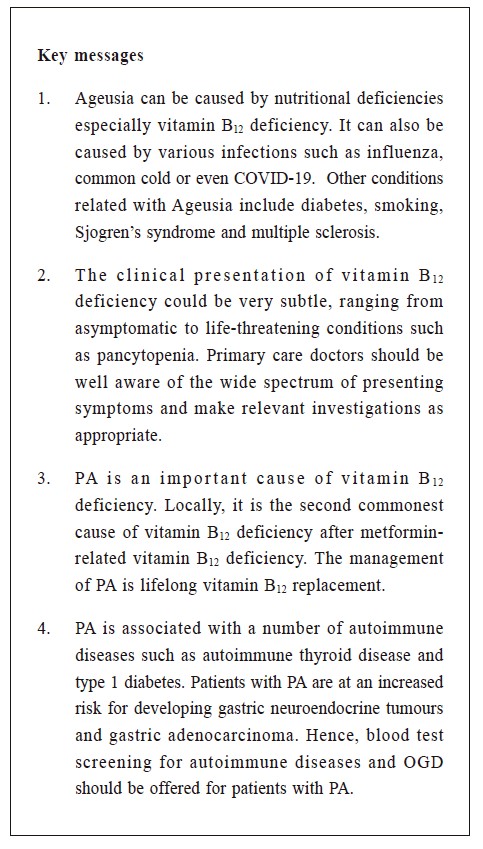
DiscussionThe clinical presentation of vitamin B12 deficiency can be very subtle especially among the elderly, therefore posing a diagnostic challenge to doctors working in the primary care setting. In our case, apart from subtle symptoms with loss of taste (ageusia), Mr. MTS did not complain of any gastrointestinal or neuropsychiatric symptoms. If not due to the presence of pallor identified on physical examination, the diagnosis of Vitamin B12 deficiency would be easily missed. Ageusia has been shown to be caused by nutritional deficiencies especially vitamin B12 deficiency. It can also be caused by various infections such as influenza, common cold or even COVID-19. Iatrogenic causes will include radiation and drugs. Other conditions such as diabetes, smoking, Sjogren’s syndrome and multiple sclerosis may also contribute. Therefore, primary care doctors should be well aware of these aetiologies and consider vitamin B12 deficiency as one important differential diagnosis when managing patients presenting with ageusia. The anaemia picture induced by vitamin B12 deficiency could be low haemoglobin only or pancytopenia when all blood lineages are affected. Pancytopenia could be a serious complication of vitamin B12 deficiency due to bone marrow aplasia. It should also be suspected in patients whose complete blood picture shows macrocytosis with hyper segmented neutrophils. Pancytopenia is a medical emergency which warrants immediate medical attention. Such patients are usually admitted into hospital to prevent the development of life-threatening infections and other medical emergencies. BMA is often offered to rule out the presence of primary haematological disorders. In our case, Mr. MTS was arranged to have a BMA immediately after his hospital admission which with the result being compatible with megaloblastic anaemia without other features of sinister haematological disorders. Once the diagnosis of vitamin B12 deficiency is confirmed, its underlying aetiologies should be actively explored. Dietary causes e.g. strict vegan diet and suboptimal oral intake are important clues. Chronic drug use e.g. high dose metformin, histamine receptor blockers or proton pump inhibitors, would also affect vitamin B12 absorption. Other conditions may be related to vitamin B12 deficiency like gastrectomy, bariatric surgery, celiac or Crohn disease or some autoimmune disorders. PA is an important cause of severe vitamin B12 deficiency, accounting for 20-30% of documented cases of vitamin B12 deficiency.4 A local study found PA was the second commonest cause of vitamin B12 deficiency after metformin-related vitamin B12 deficiency.6 Therefore, serum anti-IF antibody or anti- GPC antibody should be tested for the diagnosis of PA. Anti-GPC antibodies are very sensitive, found in 90% of patients with PA, but with low specificity, whereas anti-IF antibodies are less sensitive, found in 60% of patients with PA, but are considered highly specific.7 In our case, Mr. MTS was not a vegetarian. There were no symptoms or signs suggestive of malabsorption or autoimmune diseases. He had not been on any chronic medications. All these histories and his elevated anti-IF antibody level confirmed the diagnosis of PA. All patients with vitamin B12 deficiency should be treated, the urgency of correction depends on the severity of deficiency and associated symptoms. Parental vitamin B12 is usually the standard initial treatment for symptomatic patients. There are two forms of parental vitamin B12: cyanocobalamin and hydroxocobalamin, with the latter being retained in the body longer than the former. Hence, hydroxocobalamin is administered bimonthly to quarterly whereas cyanocobalamin is administered monthly.8 Locally, the cyanocobalamin is commonly used in the Hospital Authority. The usual regimen of parental vitamin B12 replacement is 1mg intramuscularly daily for a week, followed by weekly until the deficiency is corrected and then monthly as maintenance dose. In patient with normal absorption, oral dosing is equally effective at a dose of 1mg orally daily.6,8 As vitamin B12 deficiency caused by PA was due to anti-IF antibody that inhibits vitamin B12 absorption, parental vitamin B12 is usually used indefinitely. In our case, IMI vitamin B12 had been started immediately after admission and continued at GOPCs, his haemoglobin and serum B12 level returned to normal 4 months after presentation. PA is associated with a number of autoimmune diseases, especially autoimmune thyroid disease and type 1 diabetes. Besides, patients with PA are at 2-3 folds increased risk for developing gastric neuroendocrine tumours o r adenocarcinoma.8,9 Therefore, at least one OGD should be referred for all patients newly diagnosed to have PA. In our case, an elective OGD was performed on 28/11/2020 which was unremarkable with no evidence of malignancy. Most vitamin B12, deficiency can be successfully managed in the primary care settings. However, specialist referral would be indicated if the cause is unclear and warrants further workup, with significant complications or refractory to treatment. References
Ka-ming Ho,
MBBS, FHKCFP, FRACGP, FHKAM (Family Medicine)
Ka-yan Or,
MBChB, FHKCFP, FRACGP, FHKAM (Family Medicine)
Catherine XR Chen,
LMCHK, PhD (Medicine, HKU), MRCP (UK), FHKAM (Family Medicine)
Yim-chu Li,
MBBS, FHKCFP, FRACGP, FHKAM (Family Medicine)
Correspondence to:
Dr. Ka-ming Ho, Room 1, 8/F, Yau Ma Tei Jockey Club General
|
|