
|
March 2024,Volume 46, No.1
|
Update Article
|
Approach to asymptomatic microscopic haematuria in primary careSze-wai Yeung 楊詩煒, Pang-fai Chan 陳鵬飛, Loretta KP Lai 黎潔萍 HK Pract 2024;46:3-8
SummaryMicroscopic haematuria is a commonly encountered condition in primary care. This article aims at delivering a review of the common approach from international guidelines to strike a balance between reducing the chance of missing sinister pathologies and possibility of inducing patients’ anxiety from over-investigation.
摘要鏡下血尿是基層醫療中常見的情況。本文旨在對國際指南 中的常用方法進行綜述,從而在降低惡性疾病的漏診率和 過度檢查可能導致患者焦慮之間取得平衡。IntroductionHaematuria is one of the most common urological diseases which accounted for over 20% of urological evaluations.1 The prevalence of microscopic haematuria was estimated to be ranging from 2.4% - 31.1% depending on the features of the study population and the definition used in the studies.2 Studies showed that a cause was found in around 15% of the microscopic haematuria cases referred from primary care to specialty clinic.3,4 It was estimated that the frequency of serious urological diseases in patients with asymptomatic microscopic haematuria ranged from 0.5% to 5%.5 Therefore, it is important for primary care physicians who are the first point of contact of the health care system to recognise this condition and manage appropriately. DefinitionsThe American Urological Association (AUA) 2020 guideline defined microscopic haematuria as 3 or more red blood cells per high-power field on microscopic evaluation of a single, properly collected urine specimen.6 It is not recommended to define microscopic haematuria by a positive urine dipstick test (trace blood or greater) alone because false positive results can occur in situations including myoglobinuria, dehydration, exercise, presence of menstrual blood, or contaminants such as hypochlorite or povidoneiodine and therefore a formal microscopic evaluation of the urine is necessary.6,7 Clear instructions should be provided to patients for a properly collected urine specimen. The initial 10 ml of urine should be discarded in order to collect the midstream urine. The presence of significant number of squamous cells in the sample may signify contamination and the test has to be repeated. Catheterisation of urine should be considered in patients who have difficulty in voiding including patients with non-intact urinary tract or a Foley or suprapubic catheter or repeated contaminated samples. AetiologyThe causes of microscopic haematuria can be classified into medical or surgical causes as charted in Table 1 and it can be further classified according to the pathologies including 1. inflammatory, 2. neoplastic, 3. metabolic, 4. traumatic, 5. miscellaneous and 6. spurious.8 Table 1: Medical and surgical causes of microscopic haematuria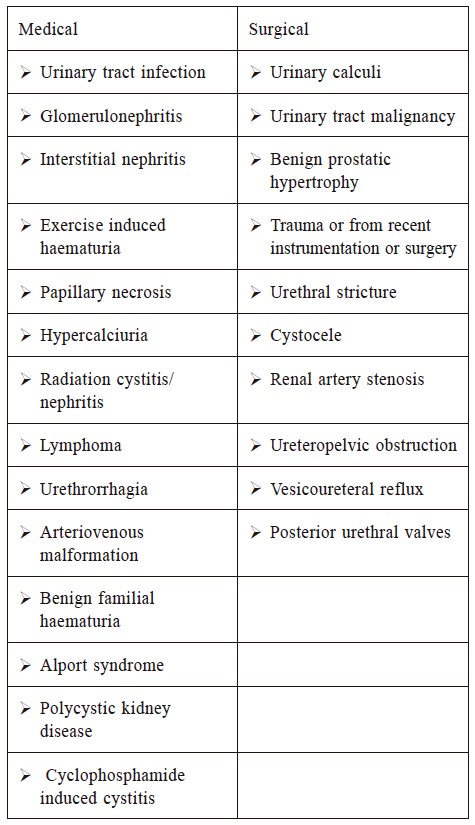
1. InflammatoryUrinary tract infection and glomerulonephritis (GN) are 2 common disease entities in this category. Pyuria or bacteriuria is commonly present in the case of urinary tract infection including pyelonephritis, cystitis, prostatitis and urethritis. Microscopic haematuria associated with urinary tract infection is usually transient. GN is a common cause of haematuria in paediatric patients. The most common type of GN is IgA nephropathy (Berger’s disease). Other less common types of GN are listed in Table 2. Dysmorphic red blood cells, red cell casts and proteinuria will present in the laboratory urine test. Renal biopsy is required to confirm the diagnosis. Table 2: Causes of glomerulonephritis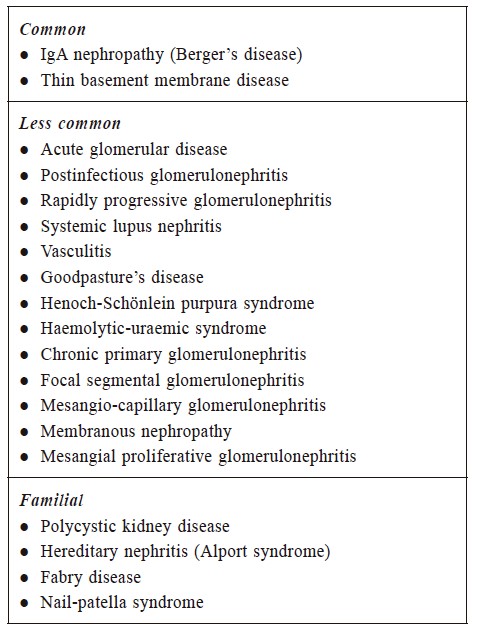
Radiotherapy for pelvic malignancies including prostate, cervical and rectal cancers can lead to radiation cystitis which may in turn lead to microscopic haematuria. 2. NeoplasticGenitourinary cancer including renal cell carcinoma, urothelial carcinoma, urethral cancer and prostate cancer can cause microscopic haematuria. Risk factors of urothelial cancer including smoking history, family history of urologic malignancies and environmental or occupational exposures to benzene chemicals or aromatic amines, etc. should be assessed from the history for risk stratification. 3. MetabolicUrinary calculi may account for one third of the cases of microscopic haematuria.8 This condition has a male sex predilection.8 The most common urinary calculi compositions are calcium oxalate, calcium phosphate and uric acid. Hypercalciuria can cause irritation of the urothelium due to the formation of microcalculi and therefore leading to microscopic haematuria. The causes of hypercalciuria include excessive calcium supplementation, hyperparathyroidism, immobility, tubular leak of calcium or increased gastrointestinal tract absorption. 4. TraumaticExercise induced haematuria can occur in sports including rowing, swimming and stationary bike riding. It was postulated that there was altered glomerular permeability and hypoxic damage to the nephron during exercise due to decreased renal blood flow and therefore causing haematuria or microscopic haematuria. Nutcracker syndrome refers to compression of the left renal vein between the aorta and proximal superior mesenteric artery which can be one of the causes of exercise induced haematuria.9 5. MiscellaneousIn a subgroup analysis of a prospective randomised trial to determine the effects of warfarin and aspirin on the heart, microscopic haematuria was detected in about 10% of patients taking the drugs, and an underlying cause including bladder cancer was detected in 10% of the cases.10 There was another study showing that 15.3% of the patients diagnosed with bladder cancer who presented with microscopic haematuria were on anticoagulants.11 The incidence of microscopic haematuria in anticoagulated patients is similar to the general population and therefore patients on anticoagulation or aspirin should be managed in the same way as the general population. Tubular necrosis can occur after the use of certain medications which include nephrotoxic agents (aminoglycosides, non-steroidal anti inflammatory drugs, anti-neoplastic drugs, etc.), analgesics, penicillins and sulfas, etc. There are also some rarer causes of microscopic haematuria including vascular malformations, Alport syndrome, benign familial haematuria etc. Details were beyond the scope of this article. 6. SpuriousBlood from the genital tract contaminating the urine sample including menstruation and sexual intercourse, can be mistaken as microscopic haematuria, therefore it is recommended to perform or repeat the urine test after menstruation has ended. Rhabdomyolysis has to be considered in suspected cases when haematuria is detected in dipstick testing. Discolouration of urine due to consumption of certain foods such as beetroot and blackberries and use of certain drugs such as doxorubicin, chloroquine, and rifampicin or chronic lead or mercury poisoning can also lead to a false positive result of the urine dipstick test.12 HistoryDetailed history is required to delineate the cause of microscopic haematuria. Particular attention has to be paid in assessing the risk factors for urothelial malignancy (Table 3) which should include smoking history, family history of urologic malignancies, and genetic or other risk factors for bladder or urothelial cancer such as environmental or occupational exposure of rubber and dye.6,8 Other important history should include age, sex, history of gross haematuria, irritative urinary symptoms, gynaecological history and medical renal disease and systemic symptoms. Physical examinationMeasurement of blood pressure is important as part of the physical examination since hypertension can be present in cases of nephritic syndrome or renal vascular disease. A genitourinary examination as guided by the clinical history including examination of the external genitalia, introitus, and urethral opening in female patients and digital rectal examination of the prostate in male patients may help identify the cause of microscopic haematuria. Table 3: Urothelial cancer risk factors (Table modified from AUA 2020 guideline)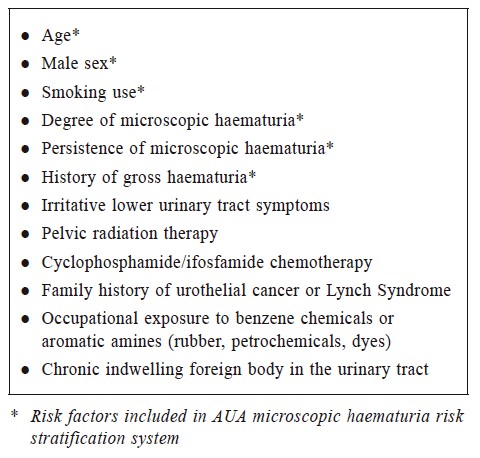
InvestigationUrological evaluationPatients with microscopic haematuria are classified as low risk, intermediate risk and high risk according to the AUA microscopic haematuria risk stratification system. (Table 4) The risk grouping system provides a general guidance in making diagnostic decisions, however, there can still be high heterogeneity among patients within the same risk group and therefore the management plan has to be individualised. Table 4: AUA Microscopic haematuria risk stratification system (modified from AUA guideline 2020)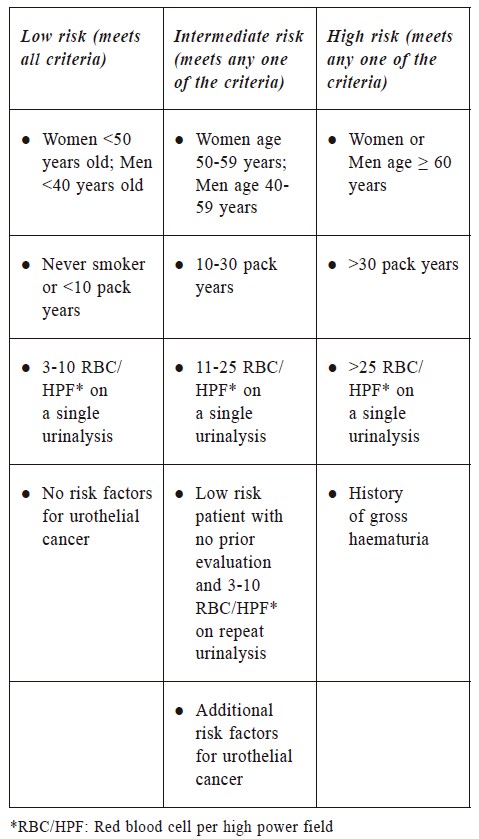
a) Low riskThe overall incidence of urological malignancy in patients with microscopic haematuria was not high with a reported incidence of 0 to 6.25% from some overseas studies.13-20 The rate of urological malignancy in low-risk group patients is expected to be low, therefore AUA suggested that shared decision making has to be made with patients about the risk and benefits of undergoing cystoscopy with renal ultrasound (USG) versus repeating urinalysis (UA) within 6 months. If patients opted for repeating UA and the result shows persistent microscopic haematuria, then their risk would be reclassified as intermediate or high depending on the level of red blood cells present in the microscopy. If the repeating UA is negative for microscopic haematuria, repeating another UA within 12 months should be considered and the patient can be released from urologic care if the repeated UA is again negative.6 b) Intermediate riskAUA recommended cystoscopy and renal ultrasound to be performed in this group of patients. Bladder cancer is the most common urological cancer detected in patients with microscopic haematuria.11,13,15,18-24 Therefore, cystoscopy is preferred for its high sensitivity in identifying bladder cancer (98%).25 Renal USG is preferred over computed tomography though it has a lower sensitivity because of the relatively low risk of upper tract urothelial carcinoma in this group of patients and the benefits of avoiding ionising radiation or intravenous contrast reaction. c) High riskCystoscopy and multiphasic Computed Tomography Urography (CTU) should be performed in patients classified as high risk as recommended by AUA.6 Magnetic Resonance Urography and retrograde pyelography are the options of upper tract imaging in patients with contraindications to performing CTU. There is consensus that cystoscopy and upper urinary tract imaging should be performed in patients with asymptomatic microscopic haematuria among the international guidelines which include the guidelines from the Dutch Association of Urology and Canadian Urology Association (CUA). However, the age threshold varies. In the guideline from the Dutch Association of Urology, cystoscopy is recommended for patients with age older than 50 and renal ultrasound is the preferred upper tract imaging, but CTU is recommended for those aged > 50 years with positive renal ultrasound or cystoscopy findings. In the CUA guidelines, cystoscopy is recommended for patients with age older than 35. Renal ultrasound is also the recommended first line upper tract imaging by CUA and CTU is suggested in cases with abnormal or inconclusive findings and symptomatic microscopic haematuria.26 
Urine cytologyUrinary cytology has a sensitivity of 52% to 80% and a specificity of 92% to 97%.27 It is not recommended to perform urinary cytology as stated in several international guidelines as the initial evaluation of microscopic haematuria 6,28-32 because of its low sensitivity and it does not provide additive information to cystoscopy. AUA recommended that urine cytology can be tested for patients with persistent microscopic haematuria after a negative workup and irritative voiding symptoms or risk factors for carcinoma in situ. Other investigationsThere are guidelines advocating the use of X-ray imaging of the kidney, ureter and bladder (KUB) together with renal USG as the initial assessment for patients with low risk of urothelial cancer. However, the limitation of KUB is that it only detects stones that contain calcium but may not identify uric acid calculi.8 Intravenous urogram is a relatively low cost and more easily accessible investigation modality, however, it is less commonly used in investigating microscopic haematuria because of its relatively low sensitivity in detecting small renal masses and pathologies in the urinary bladder and urethra. It also exposes patients to risk of nephrotoxicity with the use of contrast media.33 UA should be repeated in cases with suspected gynaecological cause of microscopic haematuria or microscopic haematuria due to urinary tract infection after appropriate treatment is given.6 Other investigations including blood for complete blood picture, serum creatinine, urine for protein, red cell casts and dysmorphic red blood cells are indicated if medical renal diseases are suspected. Follow-up and referralReferral to a urologist for further evaluation is warranted for patients with risk factors of urothelial cancer or persistent microscopic haematuria. In patients with symptoms and signs of primary renal diseases including hypertension, significant proteinuria, presence of dysmorphic red blood cell (RBC) and red cell casts or elevated serum creatinine, referral to a nephrologist is recommended.8 In the recommendation of AUA’s 2020 guideline, a UA should be repeated within 12 months in patients with a negative haematuria evaluation. Further evaluation can be discontinued if the repeated UA is negative. The decision of further evaluation should be made after discussion with patients in whom the repeated UA is positive. Further investigation is recommended for patients with previous negative urological work up who develop new symptoms including gross haematuria, increase in the degree of microscopic haematuria or new urological symptoms.6 As a primary physician, we may take part in the follow up of patients with negative evaluation. Therefore, it is important for us to know the telltale signs of underlying urological or nephrological diseases which include new onset gross haematuria, symptomatic microscopic haematuria, significant or increasing proteinuria (albumin to creatinine ratio > 30 mg/ mmol or protein to creatinine ratio > 50 mg/mmol) or estimated glomerular filtration rate (eGFR) 5 ml/min/ 1.73m2 fall within 1 year, or more than 10 ml/min fall within 5 years so that a timely referral can be made to the urologist or nephrologist.12 There is currently no local data about the prevalence of urological malignancies in patients with microscopic haematuria in Hong Kong and a standardised risk assessment tool is lacking. Future studies in our locality would be needed in order to differentiate the high-risk patients from the general population so that there would be a better use of resources and unnecessary investigations, or doctor visits could be avoided. References
Sze-wai Yeung,
FHKAM (Family Medicine), FHKCFP, FRACGP
Pang-fai Chan,
FHKAM (Family Medicine), FHKCFP, FRACGP
Loretta KP Lai,
FHKAM (Family Medicine), FHKCFP, FRACGP
Correspondence to: Dr. Sze-wai Yeung, Mona Fong General Out-patient Clinic,
|
|